|
by Rose Rohloff  A Memorial Day quote yesterday regarding veterans also exemplifies much of what has happened in healthcare over the last 10 years, regarding the focus on Population Health, meaningful use reporting, value based analysis, big data analytics-claims data, and mergers of health systems with large EMRs, with focus on reporting. “We are arguing over a statistical analysis. This is the challenge that we face in society today ,,, we are quantifying numbers because it’s easy to look at a number, and it’s not easy to look at the value of a human life. I would say to you today that (losing) one a day, one a year is too many.” Kyle Reyes, CEO, The Silent Partner Marketing When the primary focus is on data (the multiple of numbers/records-statistics), singular records and numbers or outliers are not worth the time and effort of analysts and executives. And yet, they should be as each record is a real patient, a friend, a loved one. The solution is bringing analysis down to the most base level of management with front line analysis, to coincide with first-hand observation, the voice of the patient & their caregivers/champions, and reducing the ever growing administrative overhead. Bigger is not better for addressing health and care of populations, when the focus is shifted upward with large systems where individuals are lost: Especially when the individual issues are indicative of the core problems that need to be addressed for quality care delivery. The need for P&P Reviews 
0 Comments
 Photo: Gabrielle Lurie, Special To The Chronicle: Dirty needles at UN Plaza in San Francisco, CA Numerous reports of discarded, used syringes in the streets of major cities, such as San Francisco, also necessitate being aware of 'sharp safety' in the community. Whether a street, park or playground, it is good to have knowledge of what to do, and teach your children, regarding needle-syringe safety. The following are just a couple example guidelines:  by Rose Rohloff Naloxone is an emergency medication; it is temporary and doesn't stop or eliminate opioid abuse, addiction. This week, reports were released in the media that US homes need Narcan to aid in opioid overdose epidemic, surgeon general advises Dr. Delos Marshall "Toby" Cosgrove, the previous CEO of Cleveland Clinic, spoke to a room of healthcare leaders from across the country about the Opioid Crisis in April 2017. The discussion centered around the abuse of taking prescribed medications - legally and illegally - with the current trend of NARC Parties. He explained that NARC Parties entail the supply of Naloxone (the common brand name is Narcan, used by hospital-emergency personnel as the medication to temporarily counteract a narcotic or heroine overdose.) He continued that having Naloxone allowed people to overdose, the person(s) were then given Narcan in order to continue partying. The general public needs to be aware: Naloxone has been reported to foster increased abuse of drugs by allowing revival of overdosing for continuing to take more drugs. Naloxone is the generic of Narcan. Just as EpiPen is only the delivery system and not the generic drug Epinephrine, It is important to know the difference between the brand name versus the generic drug name. The danger of advising the untrained public to distribute emergency medicine"A serious problem is many doctors and many more nurses are unaware of the different mode of metabolism of Fentanyl and Methadone. With various dosages of Fentanyl and Heroin or combinations of other opioids, the efficacy of Naloxone or Naltrexone is compromised. The general public (let alone many new doctors and nurses) do not have a working understanding of the differences in these competitive antagonists." "There may not be any impact for at least 30 minutes with a basic spray." 45 year RN, BSN, NP, MSN, Committee Member Opioid Crisis, Board of Directors Health Facility Many clinicians, let alone the general public, are not specifically trained in the proper dosage and treatment with Naloxone for the various forms and dosages of opioids and heroin. FDA Advisory Committee on the Most Appropriate Dose or Doses of Naloxone to Reverse the Effects of Life-threatening Opioid Overdose ... Sept 2016 "The effectiveness of naloxone, and thus the exposure required, will depend on the opioid dose, the potency of the opioid in binding receptors, the lipophilicity of the opioid in crossing into the CNS system and the elimination half-life of the opioid, together with patient factors (7, 26). Appendix [2] and [2a] includes further information on naloxone pharmacology. The complex pharmacology of appropriate dosing is further compounded as often the fentanyl involved is illicitly manufactured without normal procedures or controls and may be introduced surreptitiously into heroin or prescription painkillers. Reports from the field confirm the need for additional naloxone doses to reverse opioid overdoses including those involving more potent fast onset synthetic opioids." Narcan (Naloxone HCL) Use in Opiod Overdose: A Perspective4/10/2018 by Joan M. Rider-Becker, BS, PharmD, FMPARetired, Emeritus Professor, Pharmacy Practice Ferris State University College of Pharmacy Education/Training An important point for the general public who is not used to or trained in emergency medicine, this “rescue” drug is only the first step in the opioid crisis ... not the end all and be all of treatment. I would like to respond to this “advisory report” from the Surgeon General as a pharmacist, an Emeritus Professor, Pharmacy Practice from a College of Pharmacy, former President/Chair of the Michigan Pharmacist Association (MPA) and Fellow of this Association; and lastly as a chronic pain patient. I have used opioids now for chronic pain management after a car accident almost twenty-years ago. I will admit, I was taken aback by my family physician about a month ago being given a prescription for Narcan (generic name Naloxone) as a “precautionary measure” for my chronic opioid use. The form I was prescribed is a nasal formulation vs. the oral/injection form. When I took it to a pharmacy to be filled, I had to undergo “special counseling” by a pharmacist (even with my credentials) which consisted of a video on proper use and a warning that after use, 911 had to be called and I was to be taken to the emergency room for follow-up. This is the proper follow-up when someone is prescribed any rescue medication for a drug reaction. The Naloxone is only to be given when a known opioid (i.e. codeine and it’s derivatives; Fentanyl, Meperidine, etc...) is given or taken in life-threatening incidences. I was instructed, "Were you aware that Naloxone has two elimination half-lives because this drug has an active metabolite; and, were you aware that Naloxone and Naltrexone are different agents, but are easily confused." I believe giving someone this agent for overdose situations is giving a false sense of security that nothing else needs to be done. Nasal Naloxone is like putting a bandage on a cut artery. You may stop the blood flow at the moment, but the wound will continue to bleed if the wound isn’t sutured properly. Without appropriate emergency room follow up of an opioid overdose the person may die from that overdose. Many opioids vary in dose, strength, predictability and most of all drug half-life. Knowing the half-life of drugs is essential to know how long the drug is going to last in your body. Drug half-life’s, drug absorption, distribution and elimination is well covered in Colleges of Pharmacy in courses such as pharmacology, pharmacokinetics and pharmacotherapeutics. Pharmacists do not know the pharmacokinetics on every drug substance out there by memory, and we are called the drug experts. Physicians do not have nearly as much education on medications as pharmacists, yet they are the first line of treating drug overdoses in emergency situations along with the nurses, Physician Assistants and Nurse Practitioners. The general public is being provided a false sense of security by the media to carry this drug in their homes to address the opioid crisis. The public needs to be AWARE there is more to treating an opioid overdose than just squirting this agent up their nose. 
What has caused the layering of medicationsThe country is currently facing increased antibiotic resistance, opioid crisis, etc. due to our culture being conditioned in the taking of medications versus alternative treatments, or prescriptions of medications without diagnosis. A mother of a small child was recently told by a doctor as part of her son's care, "It is very important for you to teach your child how to swallow pills. Start with candy sprinkles, then swallow mini M&Ms, and then have him swallow large M&Ms so he can take multiple pills at the same time." This instruction was given to the mother without a diagnosis for her son, no plan to achieve understanding of what was causing his pain to then create a plan of care - which may or may not have needed to include medication. Consumer engagement is needed with all medications being prescribed to be fully empowered, to understand: 1) the need for prescriptions, why and when appropriate, 2) the side effects of medications to determine alternatives versus adding on more medications, and 3) to eliminate the misuse of medications without the continued layering of additional drugs. Antibiotics should only be used when the body, given time, cannot fight a severe bacterial infection. And, antibiotics should only be given out after a culture is performed to eliminate a virus as the cause, or to target the specific bacteria. Broad spectrum antibiotics should only be used with life threatening-septic issues while waiting for a culture, or there is not the ability to perform a culture.   by Rose Rohloff A middle aged male was recently experiencing severe abdominal pain, subsequently prescribed three (3) medications in two (2) weeks from three (3) different sources (an Emergency Room, a primary care doctor, a Gastroenterologist). There was no diagnosis, no care coordination within an established plan of care, no thorough instruction in the medications, with the last prescription based on a guessed misdiagnosis which worsened his pain. One prescription was a steroid with the patient being instructed to take as he needed it; the second was an offering by the office secretary blindly asking if he wanted an Epipen when he called to actually speak with the physician for worsening abdominal pain, swelling and to discuss his lab work. The common standard operating procedure (SOP) in medicine has become symptom and write a prescription, another symptom and write another prescription, etc. This SOP has lent to the opioid crisis, antibiotic resistance, as well as many other drugs being dispensed routinely with side effects causing secondary prescriptions for the side effects of the existing medications being taken. Several variables cause the use of this SOP beginning with the lack to get a full, detailed history - taking time to speak with patients - to establish a diagnosis and then plan of care, determining if simple steps are first needed such as icing and therapy for pain before opioids, or to remove foods and medications isolating side effects or allergies. Last week, I attended the HIMSS conference, the largest healthcare conference in the country, with attendees from around the world. One executive stated, "I just returned from Finland where they have an effective health system, because people live healthy, and the doctors appropriately tell their patients NO when seeking a simple, quick fix of a drug that is not needed." Reasons for the mainstream SOP? I think there are always multiple reasons for issues within healthcare. The symptom=prescription issue can be: Doctors are processing patients through with 'factory-care', Physicians receiving kickbacks from pharmaceutical companies; The lack of proper clinical training; Protocols blindly being followed without individual evaluation (e.g. Vanderbilt University study on Plavix standard for all Cardiac Cath Patients); as well as the alliance of public policy and pharma, direct consumer marketing without proper education. A healthcare executive summarized the situation well last week when stating to me, "I ultimately make the decision for my own care, with the advice of the physician. It is the doctor's role to diagnosis, and then we discuss all options, along with a plan of care, coordinated with speaking with all other involved physicians." It is important for consumers to understand the need to champion their own care working with physicians, determining what options should be used before medications (diet and some of the old fashioned home remedies still hold true), addressing underlying issues versus only symptoms, and removing or changing medications to eliminate side effects when there are alternatives. Questions to have answered: An example of direct consumer marketing lacking in education: In 2016, there was broad publication when the company Mylan raised the prices of the Epipen after State Law was passed to stock it in every school. Many individuals and groups were upset because there is not a generic offering. With proper information, the public would be educated that Epipen is the patented delivery system, not the drug epinephrine. The generic already existed in the form of a $15-$18 sterile needle. It is also necessary to establish where and when is it appropriate to stock epinephrine, not specifically the Epipen. Why are you prescribing this medication, what is it specifically doing in my system? What are non-medication alternatives, what are other medication alternatives? How long should I take this, what is the outcome? How does it interact with my other medications? What should be monitored for an outcome, side effects?  by Rose Rohloff
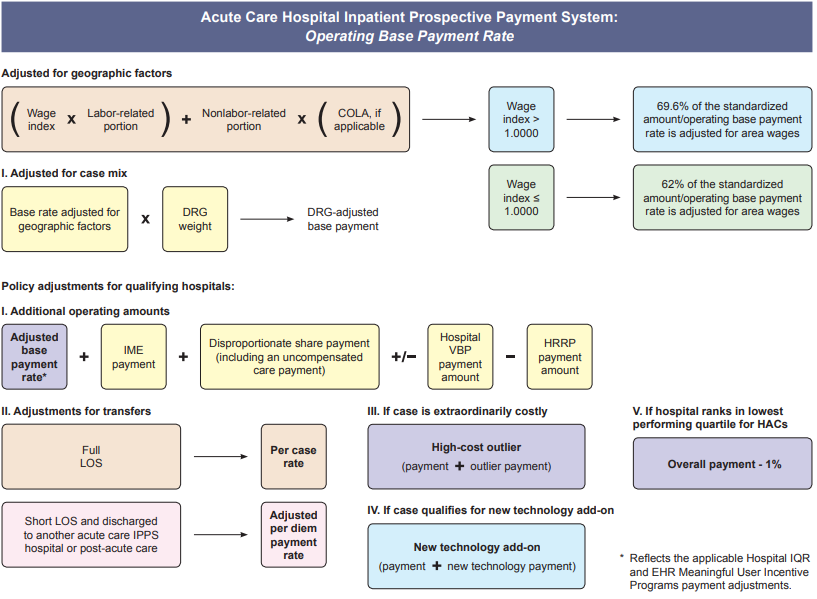
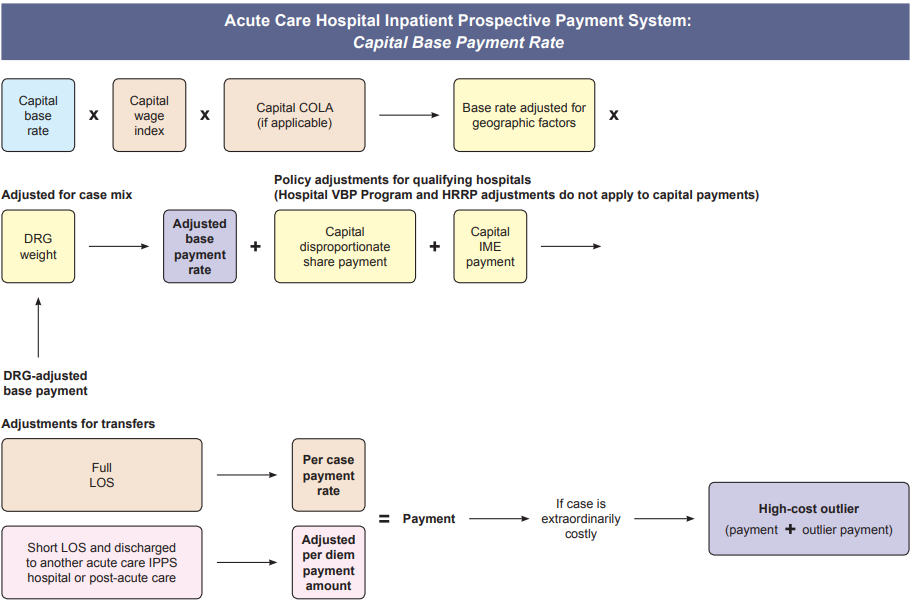
“We think sometimes we’re only drawn to the good, but we’re actually drawn to the authentic. We like people who are real more than those who hide their true selves under layers of artificial niceties.“ Elisabeth Kübler-Ross, Passion for Patients, (page 62)  by Rose Rohloff  Last week, Jeff Bezos, Warren Buffett and Jamie Dimon (I reference as the BBD solution) announced their focus for healthcare. Here are thoughts from an industry insight perspective to think about. The industry needs major shakeup for transformation to occur. BBD are technology giants focused on technology and employer offered care. This expansion will likely be predominantly that of Telemedicine, Amazon electronic medical record (EMR), and investment in technology companies. Our current system is the push for capitation (covered lives/socialized medicine, Medicaid expansion) with the focus of technology as the solution. BBD is moving this model under companies, and will impact costs. However, technology without personal and personnel intelligence with sound processes is the continued automation of bad practices and "garbage in - garbage out" data, with the potential for expanding the 'fast food healthcare' of symptom=prescription, unless we start addressing the true underlying issues impacting quality, the needed personal and personnel intelligence with mutual accountability on consumers & providers. We currently have the increasing issue of people causing accidents and walking into walls with the advancement of cell phone technology, with more and more technology trying to replace basic awareness and personal intelligence. We need to avoid the same mistake with healthcare delivery with more and more expensive technology driving up costs, without first addressing basic sense solutions. February 14, 2018 Telemedicine is a tool that can be very effective depending upon how it is used. Top 5 Ways Telehealth Will Change Under the New Federal Funding Bill, "The new federal Bipartisan Budget Act of 2018, signed into law by the President on February 9, 2018."  by Rose Rohloff The media writes about the desire for transparency with many in the public demanding posted costs for healthcare; however, the public fails to understand - healthcare is not the same as other businesses. First, in business production & marketing creates increased sales volume. Whereas, in healthcare volume is driven by need, and the primary goal of providers should be getting, keeping people healthy, in effect driving away their business. Second, the highest percent of revenue for hospitals comes from the government agency Health and Human Services (HHS), especially the Medicare division. Below is the formula for calculating inpatient payment. So unlike businesses, utilities, or other services, healthcare costs, prices and payments are not simple amounts to readily comprehend. Healthcare information has been publicly available, now is the time to educate consumers in the population of how to find and understand it to champion their care.
 by Rose Rohloff The greatest surface for cleanliness is the hands of all personnel within any healthcare providing environment. There have been arguments with the increase of hospital acquired infections (HAIs) that there needs to be expensive initiatives for reminder programs to wash hands, or to institute check list programs for clinicians to stop and go through a clean protocol before performing care. However, there is a flaw and unnecessary high expense to this approach.  Fall 2017 Hospital Safety Rating Recently, the April 2007 story of Chief Mike Day, Navy SEAL, has been recirculated. The incident involved Day being shot point blank, 27 times (11 in his vest and 16 times into his body), within a 12 x 12-foot room, the gun fight occurring within seconds at a range of ten feet. After his rifle was shot out of his hands, he grabbed his pistol, remaining in the fight, taking out the four insurgents, and then becoming stunned being hit by a grenade fragment. Upon regaining awareness, he immediately inquired if the room was clear, and then walked himself to the evacuation helicopter. In one of his interviews, he stated, “I just went to work, it was muscle memory, I just did what I was trained to do.” “… into a gun fight, I feel more comfortable in that situation, I feel more comfortable, I don’t think, I don’t have to think in that situation, I just react.” Day’s statements exemplify an important component that has been lost in healthcare training - that of muscle, or specifically, movement memory. Clinicians are supposed to be trained in school regarding the need and proper technique for handwashing. More importantly, clinicians used to have extensive clinical time working in patient areas developing the movement memory for proper hand washing, and automatically keeping in mind what is clean vs. dirty, where established sterile fields are located with maintaining of sterile gloved hands. The training was extensive and repetitive, for clinicians to automatically move appropriately in fast paced, life threatening situations - to not have to think and just act. One common, simple example is the insertion of IVs for fluid administration or needles for drawing blood. The needle or IV cannula (the needle with covered sheath inserted into the vein) is sterile, with clinicians wearing nonsterile gloves. The skin is typically wiped with alcohol to clean, and then all too often clinicians press nonsterile gloved fingers on the cleaned skin to feel for the vein; thus, contaminating the cleaned surface of the patient’s skin where insertion directly into their vein will occur. Even though the nurse/doctor is wearing clean gloves, they are not sterile, and worn to protect the clinician. With repetitive movement training, clinicians would press to find the vein before properly cleaning the skin, and clean their gloved fingers at the same time as the patient’s skin. Two frequent complaints often heard from patients, "They dug around in my arm and could not find the vein, it was so painful." "They poked me five times because they did not know what they were doing." Blood draws and starting IVs is a skill, just like shooting at a target or in high stress a gun fight, that requires proper training of technique, and more importantly, repetitive practice - especially with the understanding when someone's life depends upon it. Additionally, the conditioned good technique should be second nature to purge ALL air from needles and tubing, including from the side ports of IV tubing, to prevent the potentially fatal embolus as a hospital acquired condition (HAC). With the great reduction of hands on clinical time in schools (with replacement of online theory, population/global health, writing, and shadowing nurses), this movement memory training has been lost, with the shift of cost to hospitals for training, buying expensive monitoring equipment, or addressing the subsequent HAIs/HACs. Bringing the ingrained, repetitive movement training back to school training would instill within clinicians and CNA/PCT caregivers the instinctual, reactionary awareness of dirty versus clean or sterile, and proper IV/needle insertion, while delivering care; whether normal daily care or imminent life versus death situations – because they just do what they are trained to do without having to stop and think through quality actions.  by Rose Rohloff
As a 35-year healthcare veteran, I am a firm believer of cross-pollinating successful processes from other industries into the healthcare industry, for positive transformation. Delivering quality care will continue to be complex and challenging, with the need to leverage solutions that work. And SEAL teams are a proven efficient and effective success in the military. By rebranding PC teams and the team process, expanding with additional SEAL successful methods and approaches, we can create the Healthcare version of SEALs (sea, air, land), as APAC Teams (acute, post-acute, and community) - expanding the process to operate in every environment versus only in facilities, for enhancing the quality of care of high risk patients versus limiting to end-of-life cases. The following chart displays characteristics of SEALs, obtained from several former SEAL, special operation personnel, and military officers; with several of the attributes emulating characteristics regarding the successful palliative care (PC) team process.
* https://www.navy.com/dam/Navy/Navy-IMG/Downloads/pdf/enlisted/seal-brochure.pdf ** http://www.nsonswmentor.com/Navy-SEAL.html Within the industry, PC is still aligned or mistaken with hospice, as demonstrated in the following two scenarios. Recently, a viral video was circulated and applauded, Australian paramedics fulfill dying woman’s wish to go to the beach, telling the story of a Hervey Bay crew transporting a patient to the palliative care unit, but she wished she could, “Just be at the beach” instead, and so the crew drove to the beach to provide her peace, based on her wishes of quality of life. This story is lovely regarding true care of a patient. Additionally, in April of this year I attended the Becker’s Hospital Conference in Chicago with the top leaders in healthcare, with a wonderful presentation about business analytics regarding palliative care, end-of-life. Both stories demonstrate clearly that palliative care is still being confused with hospice, or limited to a specific unit definition, instead of the effective use of the team process use with complex and/or chronic conditions.
However, what is it continuing to do to their brains having more medications and anesthesia, while it may not be improving their actual quality of life?” With APAC team coverage, a non-end-of-life case can be reviewed with a sound plan of care based on the desired quality of life for the patient and family. The PC coverage in the community has been focused on cancer patients, with a high focus on children. With the demonstrated cost savings and positive outcomes with The value of palliative care teams (HFMA, March 2013), the community coverage can be successful for individuals with multiple comorbidities, such as diabetes with congestion heart failure and hypertension; as well as elderly who are being targeted when ‘sundowning’ with fraud scams, or confused with medication regime, and those with family living in other states who are their primary support system/durable power of attorney. It is daunting, emotionally and financially, for the families of high-risk consumers to search out the various interdisciplinary resources such as dieticians, social workers, case managers, pharmacists, nurse practitioners, and spiritual counselors. APAC teams would also address the necessary information gathering for determining the real issues of consumers, for example, who needs dietary changes or removal of drugs with side effects before being prescribed new medications by physicians, causing even more side effects or noncompliance, and self medicating or opiate abuse. PC teams can be expanded to APAC teams utilizing the successful palliative care process across the care and health continuum, eliminating the end-of-life association, and differentiating from the terminally ill care of hospice. Just as SEALs operate in every environment (air, sea and land), APAC teams can be an extension of PC teams to be the quick, nimble action teams in all settings, especially the community, for patients with complex and chronic conditions.  by Rose Rohloff  Sleep apnea affects about 18 million people. This condition is linked as a major contributor to atrial fibrillation as well as multiple other health issues. Individuals have previously had to go to sleep centers for diagnosis, which is time consuming, and people generally do not sleep well in a foreign environment. "The Mayo Foundation for Medical Education and Research (Mayo Clinic) has purchased the WatchPAT device, an FDA-approved sleep apnea home testing device developed by Israeli medical diagnostics company Itamar Medica." nocamels -- Israeli innovation News WatchPAT is an FDA-approved portable diagnostic device that uniquely uses finger based physiology and innovative technology to enable simple and accurate Obstructive Sleep Apnea (OSA) testing while avoiding the complexity and discomfort associated with traditional air-flow based systems.  by Rose Rohloff

The lab model has great benefit, and feasible when costs are not prohibitive, especially avoiding a doctor's office visit when only ordering labs, or if one wishes to bring any abnormal readings then to the doctor's attention. With the many lessons learned from an aborted (shady) startup, marketed to disrupt the healthcare industry with its counterfeit technology, the direction for having consumer-driven as the process should not be overlooked - and actually be revisited to expand upon the great health ownership model of good disruption to healthcare.  A research letter published in JAMA Internal Medicine claimed patient satisfaction-based ratings are associated with patient outcomes, but a recently released study from Quantros disagreed, saying the letter's findings are misleading and may lead patients toward poor clinical outcomes. Ms. Rohloff, a 35-year healthcare veteran with experience in nursing, business and information systems, spoke with Becker's Hospital Review about providing consumers with more detailed evaluation of quality care delivery. [read more]  The healthcare industry has used perioperative morbidity and mortality reviews (M&Ms) for blunt evaluations, to continuously improve the understanding of and performance in surgical intervention. Since the industry touts Population Health and Patient Engagement as top initiatives, health systems can use the successful process of M&Ms to perform Population Health and Patient Engagement reviews (P&Ps) of individual cases, for ensuring quality care processes. [read more] Published Becker's Hospital Review.  "Those in healthcare are there for the patients, the patients are not there for them. If we stopped for a moment to view the actual words 'patient,' 'health' and 'care,' there is no 'I' in either 'health' or 'care,' only in the word 'patient.'" Those in the healthcare industry tout the idea of prioritizing patients by using phrases such as "patient-centric" and "patient engagement," and yet current data trends suggest the contrary is happening. Instead, motivation based on self-interest continues to permeate care delivery. Here are three trends in the healthcare industry that work against patient-centered care. [read more] Published Becker's Hospital Review.  Upon reading the article "Must have bachelor's degree: Hospitals' new requirement for nurses" concerning a report published by The Wall Street Journal, I wanted to provide perspective from experts with first-hand experience in the industry addressing points within and not included in the Wall Street Journal report. [read more] Published Becker's Hospital Review “I spoke to more than 40 people for the story and heard many of the points you raise, unfortunately I could not include every nuance in a 700-word story. All the best, Anna” WSJ journalist 
The intention of my June hfm business intelligence (BI) column* was to gauge how well the industry has standardized definitions by conducting an informal survey of leading providers, consultants, and vendors. It was refreshing that so many respondents were eager to participate, and they showed care for wanting to improve the industry. After reviewing a wonderful broad range of great responses, one striking point stood out: The healthcare industry has not clearly defined Population Health. Lacking a uniform definition makes it difficult to define when healthcare has succeeded, to establish key performance indicators (KPIs) for monitoring progress, to determine which solutions lead to that success, and most important to educate the population on what initiatives and goals are being offered to help them. After performing the industry survey, I thought about one important step healthcare leaders have not done - ask the consumer, those individuals who make up the population - what is the public’s understanding or desire for Population Health. With this in mind, I wanted to conduct a survey of 100 non-healthcare people across the country, of various ages, a range of industries, and regardless of political affiliation. Each person was asked:
Many people looked confused upon being asked those questions and stated they have never heard the term before, while others provided an immediate description. Although the survey showed the lack of any definitive definition, and verified the general lack of understanding of the concept, it showed how much the public wanted to talk about Population Health, with several people engaging me in conversation to find out what the industry is doing and asking, “What is the actual definition?” *https://www.hfma.org/BIgoals/ Survey ResultsOverall Breakout by Age, Gender, Industry & Definition Grouping 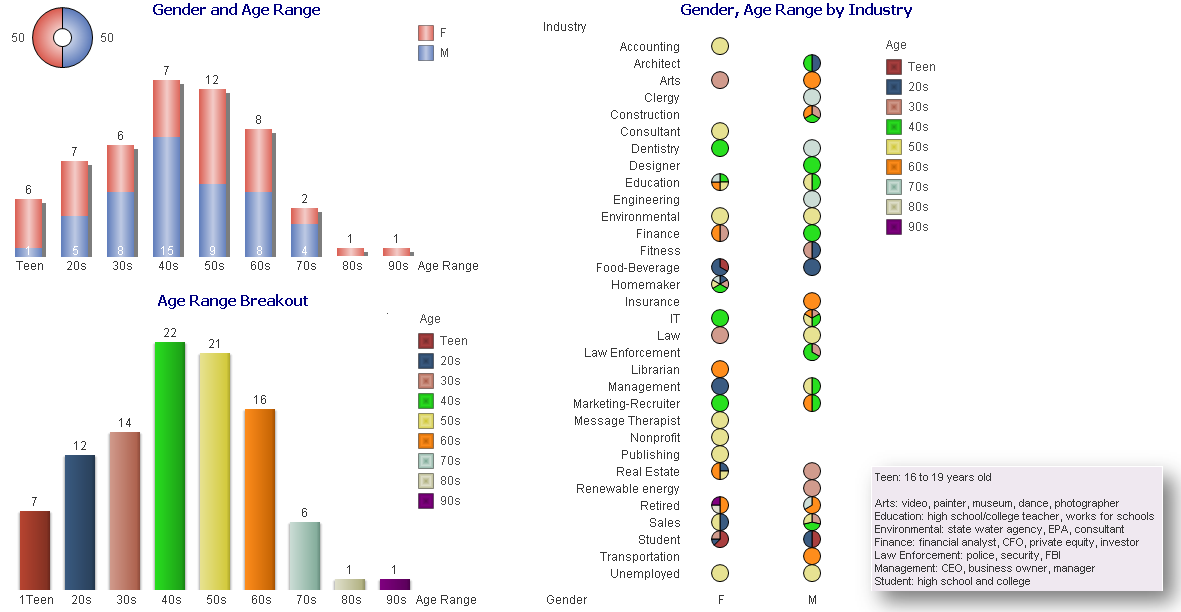 Exhibit 1: Gender 50:50, Age Grouping, and Age Group by Industry and Gender Have you heard the term Population Health before? Yes/No 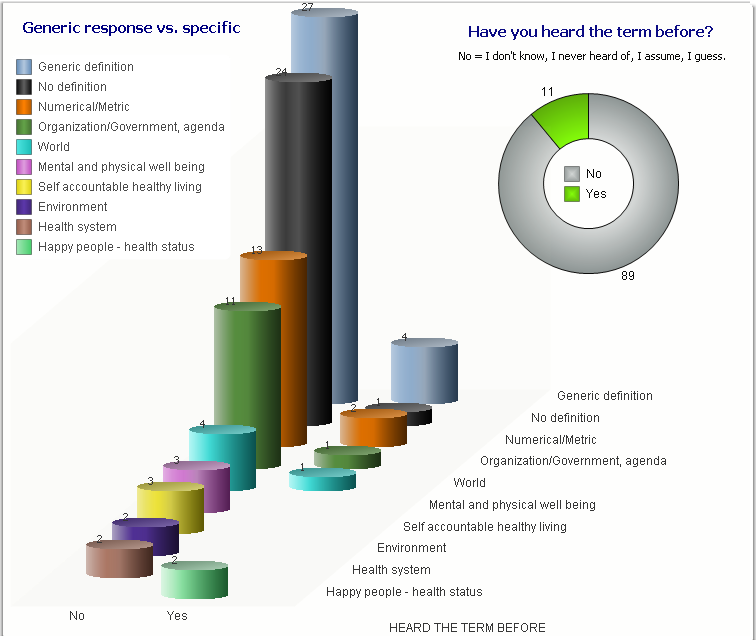 Exhibit 2: , Answers Grouped into Categories Have you heard the term Population Health before? = Yes What is your understanding of the definition? 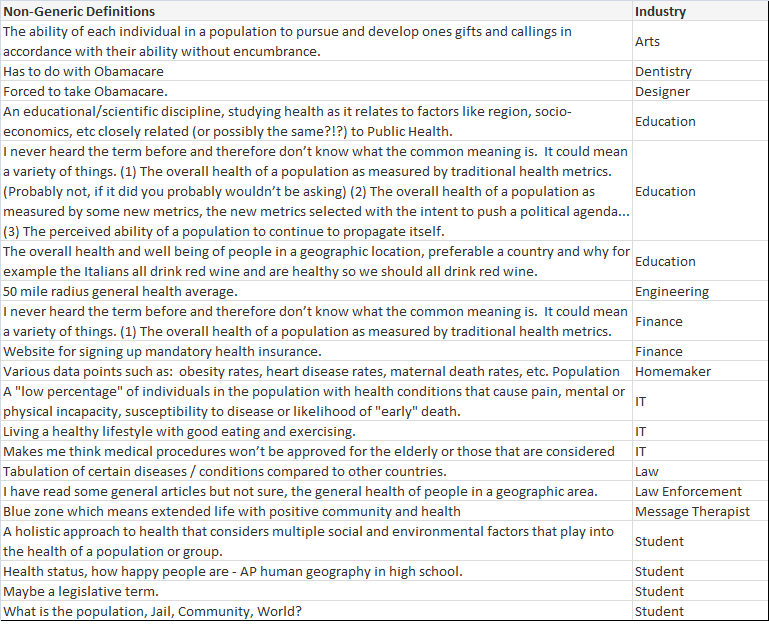 Exhibit 3: non-generic definitions provided according to industry. 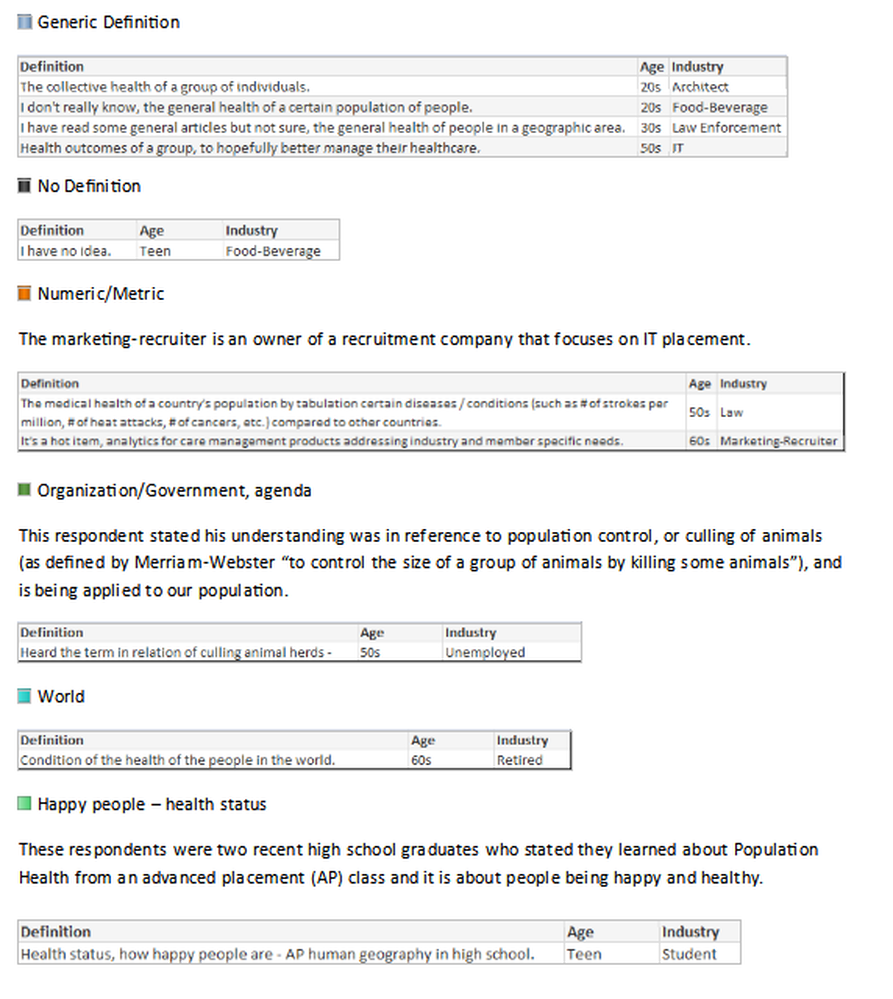 Exhibit 4: Demonstrated confusion about definition - answers grouped into categories. The majority of responses were vague, generic definitions; the following are non-generic definitions provided according to industry.
In the hfm article, I proposed that the industry standard definition needs to include “a partnership with the community of health seeking persons” including “putting data into the hands of patients and encouraging them to share accountability for health outcomes by choosing healthy lifestyles, following health regimens, and seeking health education.” As the public survey shows, we in the industry need to ascertain their understanding, and have a collaborative relationship for population health management with a clear definition and public education regarding solution offerings. Have you heard the term Population Health before? = No What would be your understanding of a definition? It was refreshing to come across so many in the public who have the desire for health care discussions and want to understand what is transpiring with the changing environment. It was additionally refreshing to see how many want the right information to make knowledgeable decisions. 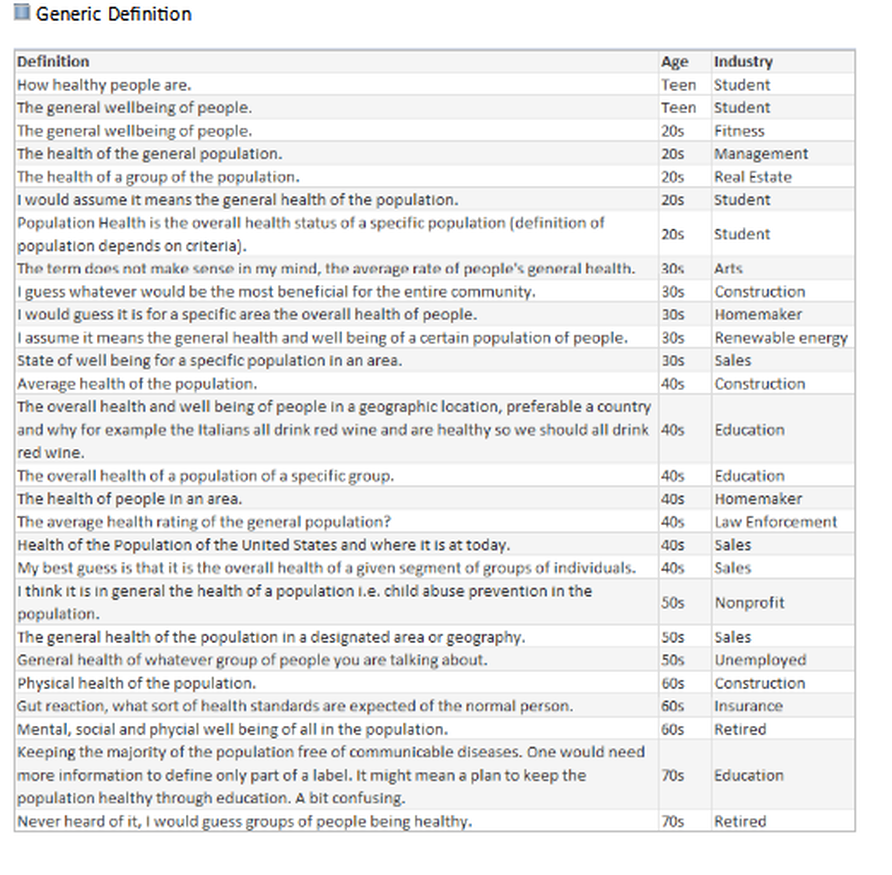 Exhibit 5: No response general 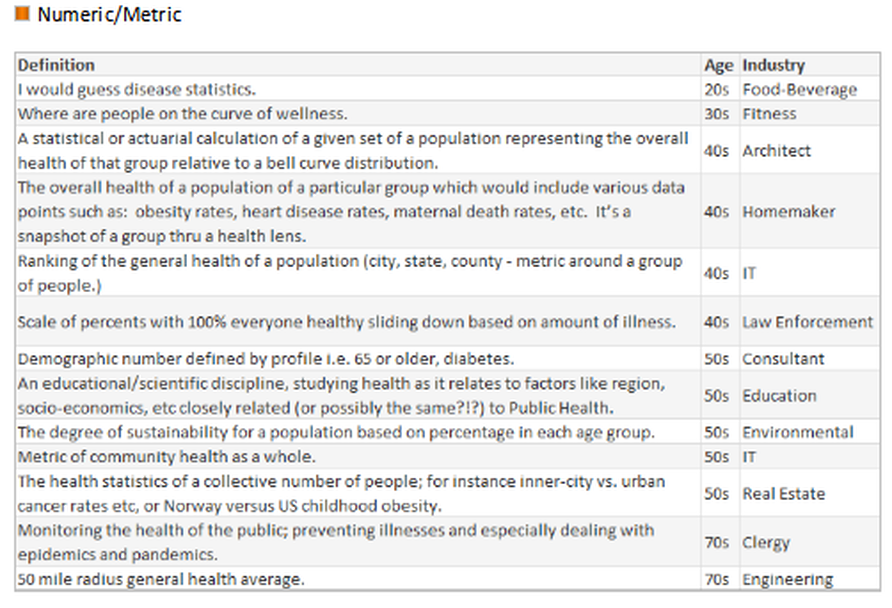 Exhibit 6: No numeric/metric 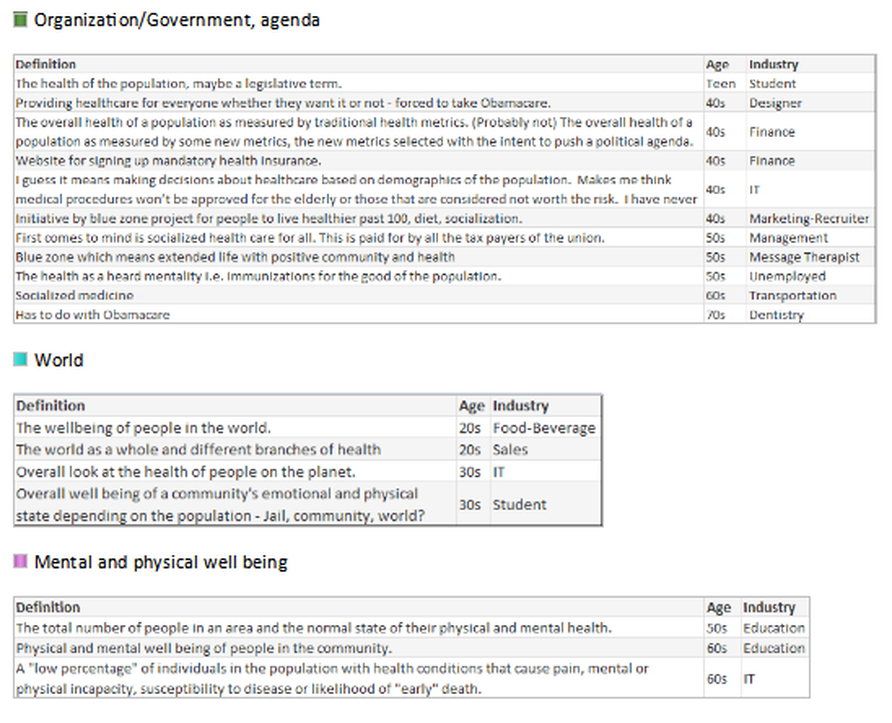 Exhibit 7: Org, World, Mental 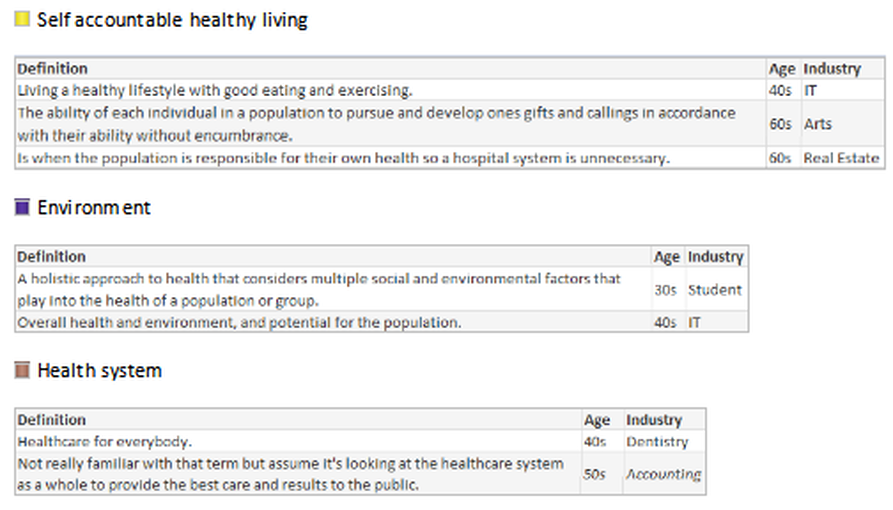 Exhibit 8: Self, Environment, Health As a general finding, respondents between the ages of: 16-17 Wanted to convey input. 18-20 Had general apathy regarding the topic and generic input without additional inquiry. 30-40 Showed the highest desire to participate and have conversation regarding – the largest group with children and facing older parents with increased health concerns. 50-60 Wished to participate with continued conversation regarding what is happening in the industry with more defined ideas of what the term means. 70-90 Were an active and health conscious group being very productive in their communities and had a desire to learn about the topic. Summary
It is time to go back to a care for healing, or as the quote in the movie People Will Talk, "I heal sick people" environment again, not with a general population, socialized medicine approach, but an individual focus once more for sustaining health. Addendum: all answers by age groupings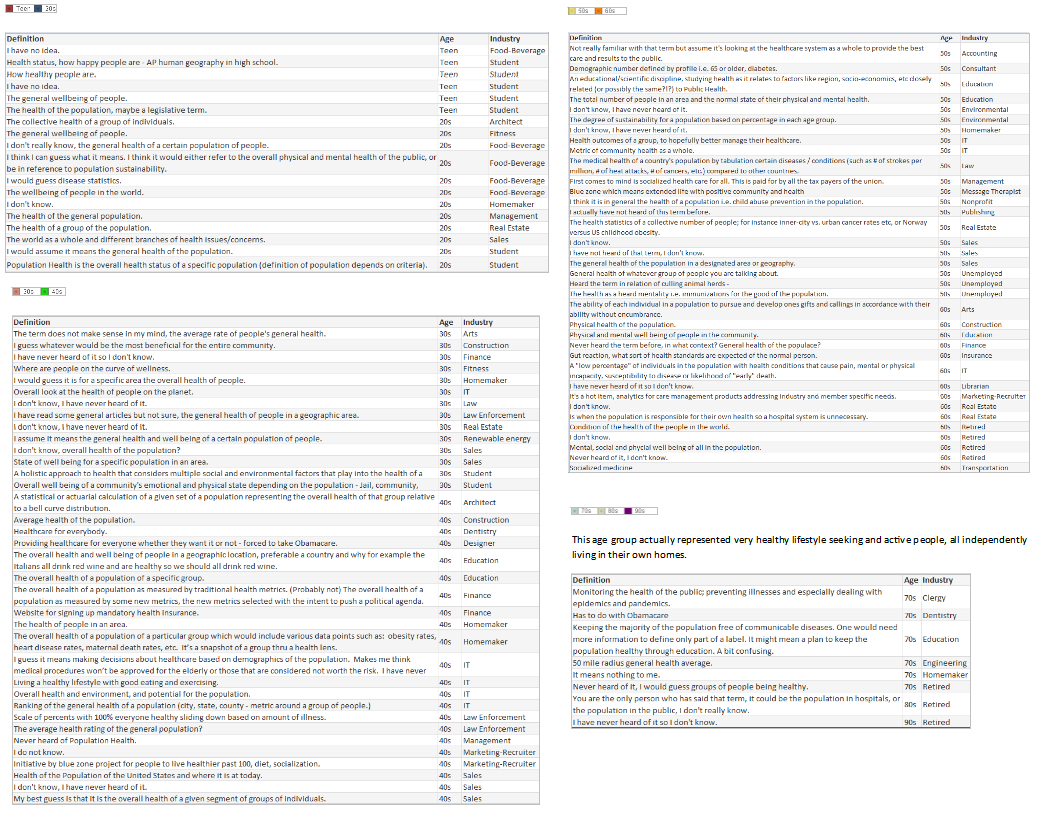  |