Engagement Awareness
for Championing Care
Real Stories from Real People
patients & families having a voice, sharing experiences at the ground level
|
I went to the doctor, had a diagnosis that I needed a commonly done elective surgery - it was not urgent, emergent as in life threatening. The surgeon stated it needed to be delayed because of Covid. After elective surgeries were being scheduled again, the surgeon's office stated I needed to come back in and be assessed all over again before they could reschedule. When I called the office, I asked if they were going to bill me for a second co-payment charge, when I was already diagnosed, and I am being told to come back in due to their cancelation; and was put on hold after the admin stated she had no idea.
0 Comments
Hospitals are classified as acute care centers for treatment of acute conditions, so I can go home and recoup/rehab. Emergency rooms (ERs) are part of Emergency Departments (EDs) as the point of entry to be stabilized for admission as an inpatient or go immediately to surgery. If it is not life threatening or severe, I should first go to an Urgent Care Center (UCC).
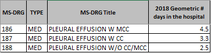
My dad was readmitted into the hospital. They needed to plug something? for a pleural effusion, first needing to get his blood work correct from his blood thinners (10?). They said his blood work was good Friday night but because it was a holiday weekend, they were not going to do the procedure until Monday. He was in the hospital for seven days.
My mom was in the hospital for kidney stones and they did a great job coming in regularly to ask how she was doing and managing her pain every few hours. Her only complaint was the ten pounds of fluid they put on her.
An elderly woman with confusion, vomiting, weakness and malaise is taken to the ER, admitted for a three day hospital stay and discharged. She was given a patient experience survey with the response, "Oh, they took such good care of me, they were all so nice."
|