"Ninth Circuit Court Full Details... read each bullet point baby! (1) The court ruled that the district court misapplied the 1905 Jacobson case because LAUSD relies on a drug that Plaintiffs plausibly alleged did not prevent the spread of the virus. (2) LAUSD has changed its mind about requiring the vaccine and therefore, the case cannot be mooted because LAUSD has proven it will just enact it again later. (3) The court said, "But even if the materials offered by LAUSD are subject to judicial notice, they do not support rejecting Plaintiffs’ allegations. LAUSD only provides a CDC publication that says “COVID-19 vaccines are safe and effective.” But safe and effective for what? LAUSD implies that it is for preventing transmission of COVID-19 but does not adduce judicially noticeable facts that prove this." (4) "Pursuant to more recent Supreme Court authority, compulsory treatment for the health benefit of the person treated—as opposed to compulsory treatment for the health benefit of others— implicates the fundamental right to refuse medical treatment. Plaintiffs’ allegations here are sufficient to invoke that fundamental right. Defendants note that the vaccination mandate was imposed merely as a “condition of employment,” but that does not suffice to justify the district court’s application of rational-basis scrutiny." (5) MUST READ THIS..."In Washington v. Glucksberg, 521 U.S. 702 (1997), the Court explained that Cruzan’s posited “‘right of a competent individual to refuse medical treatment’” was “entirely consistent with this Nation’s history and constitutional traditions,” in light of “the common-law rule that forced medication was a battery, and the long legal tradition protecting the decision to refuse unwanted medical treatment.” Id. at 724–25 (citation omitted). Given these statements in Glucksberg, the right described there satisfies the history-based standards that the Court applies for recognizing “fundamental rights that are not mentioned anywhere in the Constitution.” Dobbs v. Jackson Women’s Health Org., 597 U.S. 215, 237–38 (2022). The Supreme Court’s caselaw thus clarifies that compulsory treatment for the health benefit of the person treated—as opposed to compulsory treatment for the health benefit of others— implicates the fundamental right to refuse medical treatment." https://cdn.ca9.uscourts.gov/datastore/opinions/2024/06/07/22-55908.pdf… 
0 Comments
by Rose RohloffTHE ORIGINAL HIPPOCRATIC OATH ALTERED & EXPANDEDCaring for health will not improve until we bring back oaths: binding testimonials for committed healers. The privilege and honor of being in charge of lives with integrated souls is not a job; it is a calling. We, individual Christians - not schools, governmental agencies or regulatory bodies - hold each other to the highest standards. And, oaths are taken and upheld by individuals. The following expansion on the original Hippocratic oath is for MD/DO/DC, PA, RN/LPN, Naturopath, Therapists, etc. anyone within the industry of healing. I (name) will perform my duties with faith and trust in God as my guide, and continually learn as long as I perform my duties. I will impart a knowledge of the art of healing, mentoring and teaching those I serve. Above all else, I will abstain from whatever is deleterious, mischievous, malfeasance or unjust to those being treated, and I will not break what is not broken, for that is doing harm. Clinicians post degrees; what about posting the oath they abide by, adhere to, and practice within its ethos?  by Rose Rohloff
 Exhibit A: EcoHealth Alliance proposal to DARPA page 3; intention = GOF as per DARPA 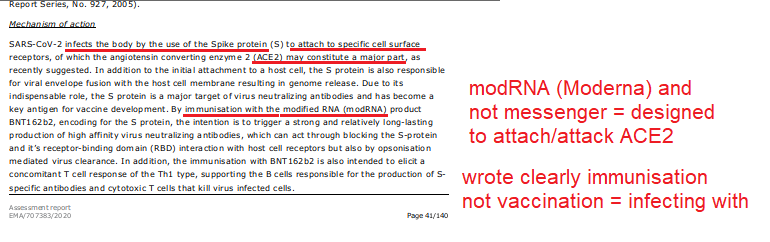 Exhibit B: Pfizer document components of the shots 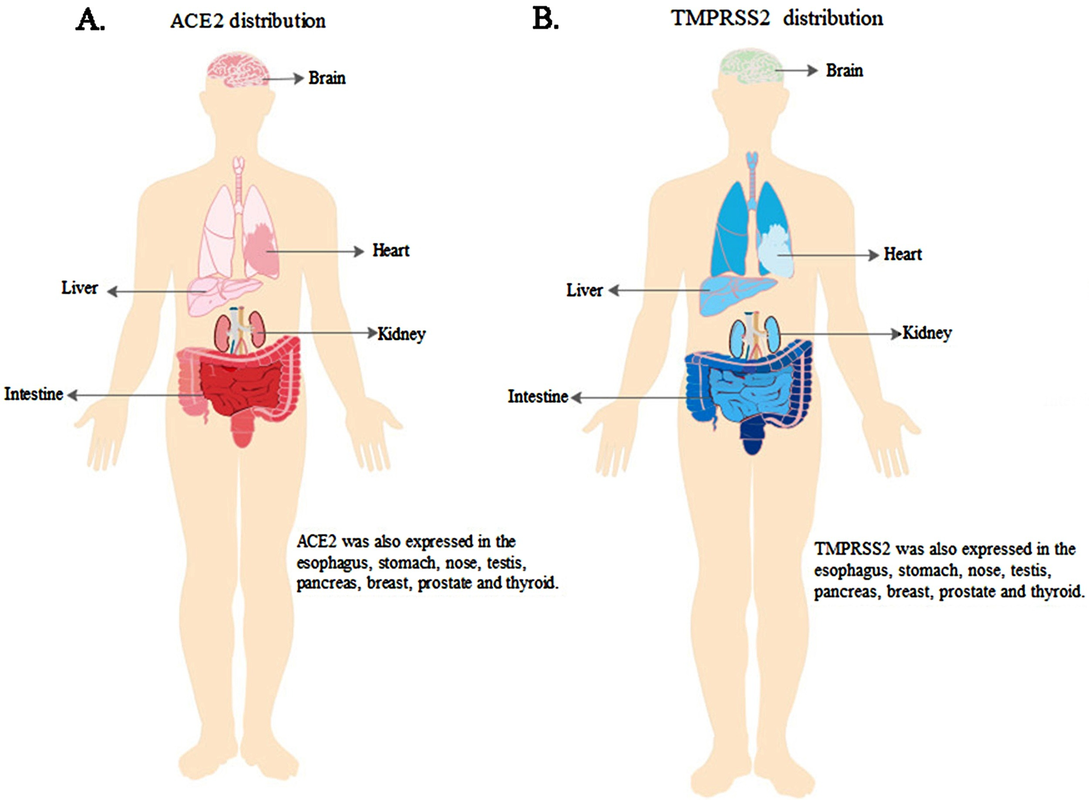 Exhibit C: ScienceDirect "ACE2, TMPRSS2 distribution and extrapulmonary organ injury in patients with COVID-19" Nov 2020 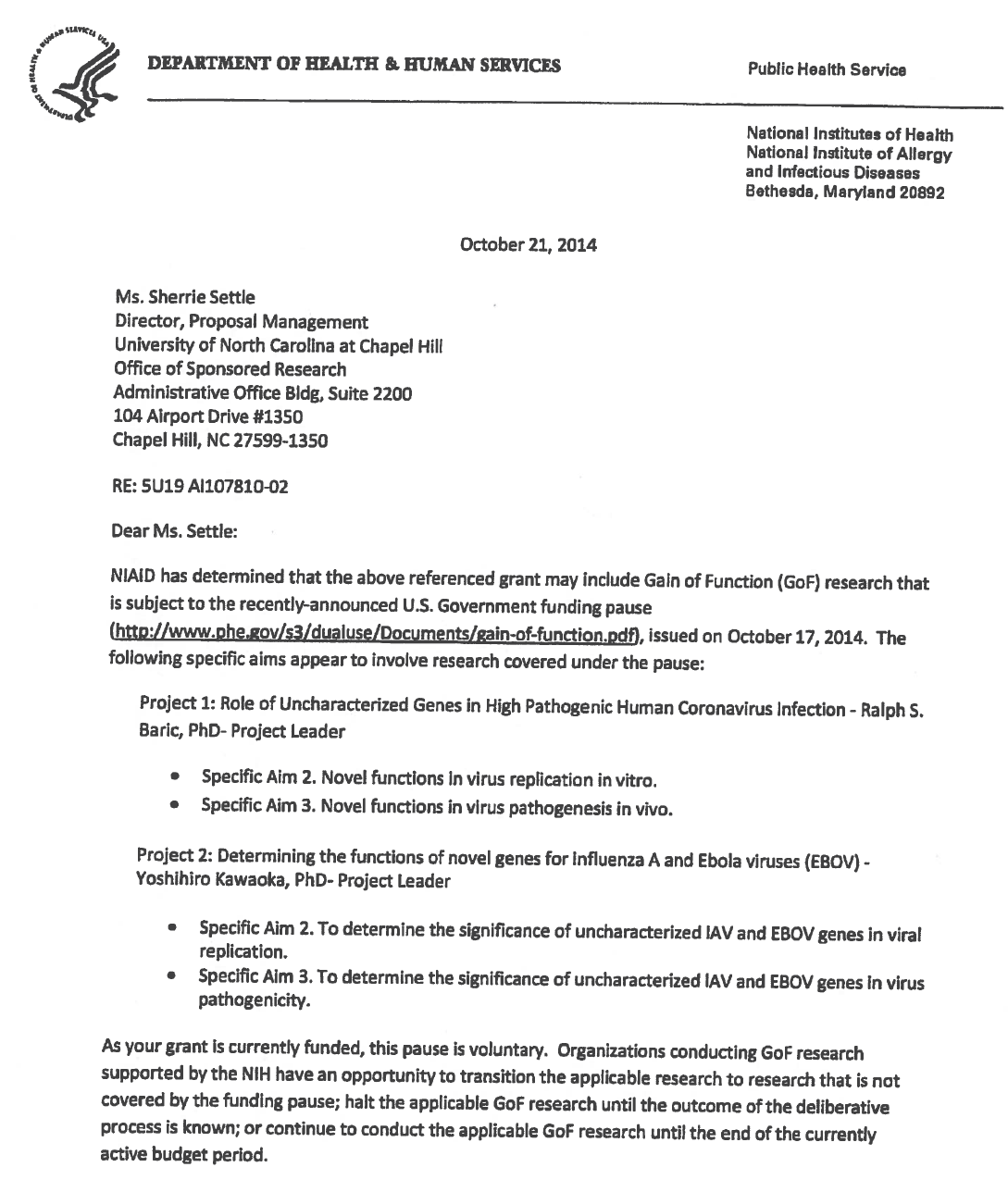 Exhibit D: Un of NC letter GOF * Date: written 2015 posted 2016 * Not natural: chimeric infectious clones, GOF  Exhibit E: Baric, Univ NC, Chapel Hill - 2016
The 1974 Research Act was created in entirety from the Belmont report, and put into place to prevent the Government, it agencies or representatives, military and private companies, from violating an individual's freedom: by forcing, tricking or coercing persons for research, testing and administration of unknown injections/materials, and experimental procedures. This law was enacted after a century long track record of precedence including, and not limited to, the following:
Demonstrated lack of Respect for Persons and their protections in violation of 1974 law. 1- Autonomous agents, individuals capable of deliberation about personal goals and of acting under the direction of such deliberation. The Government and companies have to give weight to autonomous persons' considered opinions and choices, and cannot obstruct their actions and judgments, nor deny individual freedom to act on considered judgments, and cannot withhold information necessary to make a considered judgment. Necessary information includes - but not limited to - all medical opinions by established, industry experts, health status, the necessary assessments, labs, with close monitoring of physical lab and test follow ups of each and every autonomous persons as part of clinical research and testing, along with full documentation of testing, efficacy, use of chimera for research and testing, any and all conceivable side effects, and interactions of conditions.
 2- persons with diminished autonomy are entitled to added protections. Violators to the law have been marketing to the most vulnerable, including the immature and the incapacitated who were in need of extra, added protections, even to the point of excluding them from any injections or procedures which may harm them; violating added safety precautions for children, elderly, or those with diminished capacity. Informed consent - must include full disclosure of ALL contents to be injected, any and ALL possible side effects (which can be several pages long), how those persons are individually to be closely monitored, safety guidelines, and above all the right to say no before or at any time, and full reporting of all individuals regarding their safety monitoring/labs/assessments, and any and all side effects. By promoting COVID shots all still under clinical trial/research, and coercing with careers/jobs, inability to travel, etc. in order to take the shots, this law is being violated through: lack of informed consent, lack of protections of autonomous persons, and/or illegally acting as IRB safety board members marketing to those not autonomous and capable of self-determination, with higher standards of protection to be invoked, and assuming the role for their safety. The maxim "do no harm" has long been a fundamental principle of medical ethics. Claude Bernard extended it to the realm of research, saying that one should not injure one person regardless of the benefits that might come to others. An agreement to participate in research constitutes a valid consent only if voluntarily given. This element of informed consent requires conditions free of coercion and undue influence. Undue influence also includes offers of an excessive, unwarranted, inappropriate or improper reward or other overture in order to obtain compliance. Also, inducements that would ordinarily be acceptable may become undue influences if the subject is especially vulnerable as in the case of targeting children, persons with limited capacity, and elderly with elements of mental defect, or instilling fear. Short term morbidity and mortality cases from the shots are well reported and known, such as death, myocarditis along with spontaneous cardiac arrest with no warning, debilitating neurological conditions, etc. And, there is no means yet to determine mid and long term effects because Phase I trials have not been competed, let alone Phase II and III - which is vital information in order to determine informed consent. Injustice has been performed with companies and government representatives, by involving vulnerable subjects, including the young, those unable to fully comprehend with all necessary information, and scaring parents with compromised capacity for free consent. In addition to lack of individual, tightly scheduled, continual monitoring and follow ups, autopsies of all persons involved in this trial participation should be conducted for reporting by the pharmaceuticals companies for any and all persons who received the shots, as well as labs determining efficacy and detriments (as examples, antigen creation, D-dimer, Pulse Cardiac and Troponin Tests) for all those who were coerced or unduly influenced to participate in research. This law was created to protect people from government abuse through experimentation. The government cannot arbitrarily dismiss components, create resolutions or stipulations to supersede the law, as to invalidate its protection of individuals from them, including, but not limited to Health and Human Services (HHS) Center for Disease Control (CDC), Food and Drug Administration (FDA), National Institute for Health (NIH), etc. and pharmaceutical companies, etc. Persons have been illegally acting as members of, or bypassing, IRB safety review and monitoring of each and every person receiving injections, with open undue influence and coercion, to participate in Covid injections. Coercion has been especially directed to the diminished autonomous, children and elderly, through TV ads, library recordings, verbal encouragement, schools or other public venues acting as government agents, and/or clinical researcher recruiting participants, and/or illegally as untrained IRB member who is not following up to ensure safety of the people they recruited, coerced or used undue influence. Overall lack of informed consent has become too often common practice across the healthcare industry, including people being given consent forms hours or minutes prior to surgery; no alternative treatments or lifestyle-nutrition changes prior to medications begin prescribed, and undue influence to intubate or perform surgery on patients in lieu of alternative treatments.
Lawsuits for unconstitutional violation of laws regarding shotsPosted by Brian Ward on Twitter Guess what? Defendants in our lawsuits no longer argue that they had a right to mandate EUA drugs due to their state's at-will employment doctrine. That the EUA drugs can be mandated. That they had the authority to even issue the mandate. Why? Read the 127 pages, and then you'll understand that it was a legal lie from the beginning, but due to the novelty of the laws, no one knew of them. As courts have stated, "sometimes laws take naps," and these laws never showed up for work until now. https://coloradomedicalfreedom.com/wp-content/uploads/2023/08/Stamped-Final-Complaint.pdf full document https://coloradomedicalfreedom.com/wp-content/uploads/2023/08/Stamped-Final-Complaint.pdf page 127 C. the Secretary has no “authority to require any person to carry out any activity that becomes lawful pursuant to an authorization under this section…” 549. In 2005 Congress passed the PREP Act94 which provided the following regarding preemption of state law: (8) During the effective period of a declaration under subsection (b)…no State or political subdivision of a State may establish, enforce, or continue in effect with respect to a covered countermeasure any provision of law or legal requirement that— (A) is different from, or is in conflict with, any requirement applicable under this section; and (B) relates to the…administration…of the covered countermeasure, or to any matter included in a requirement applicable to the covered countermeasure under this section or any other provision of this chapter, or under the Federal Food, Drug, and Cosmetic Act [21 U.S.C. 301 et seq.]. 550. Therefore, via the PREP Act and 21 U.S.C. §360bbb-3, Congress expressly prohibits Defendants from: A. interfering with the authority of the Secretary, B. establishing a condition not authorized by the Secretary, C. establish conditions contrary to the Secretary and the congressional statute under 21 U.S.C. §360bbb-3, D. mandate participation in any 21 U.S.C. §360bbb-3 product or PREP Act activity, E. interfere with an individual considering participation in a 21 U.S.C. §360bbb-3 product or PREP Act activity, F. penalize a person refusing to participate in a PREP Act product or activity or 21 U.S.C. §360bbb-3 product. 551. The executive branch of the United States Government purchased all COVID-19 licensed and EUA drugs using federal funds. Congress expressly prohibits the federal government Brian Ward @GodsRiddles Nov 1, 2023 Breaking…Gov Gavin Newsom and Kaiser have been sued in federal court for requiring healthcare workers to inject an experimental drug into their bodies as a condition to sell their labors in the marketplace. The requirement violated the workers’ Equal Protection of Laws and Due Process rights. Moreover, Kaiser signed a contract with the CDC promising not to mandate participation but did so anyway. Kaiser and Newsom fraudulently concealed the fact that nurses would be required to forfeit litigation rights if they incurred an injury from the use of the experimental drug. The California Nurses union stood by and refused to stop Newsom’s tyranny, leaving members without representation. Governor Newsom perpetuated the greatest assault on the US Constitution in the state’s history and the CA AG did nothing to prevent it. Worse yet, is that CA and Kaiser already had an agreement with HHS promising to never place an individual under a sanction for refusing to inject federally funded experimental drugs into the body. Legal Fact: medical providers have dual roles in relation to their employees. An employee can be a patient and an employee. Should a hospital mandate the use of a drug under the PREP Act as a condition of employment and the patient is injured then the patient would find it difficult to sue the medical provider for that injury. However, the employee has the right to seek compensation irrespective of the PREP Act because it’s an on the job injury. Of course this opinion does not account for the laws of all 50 states but demonstrates why one should seek legal advice immediately upon sustaining an injury. This is not my opinion but the chief judge of the 11th circuit who wrote a slip opinion when he was AL AG denoting the company is liable for vaccine injuries because the company believes the vaccine would benefit the company. Last edited10:55 AM · Nov 10, 2023
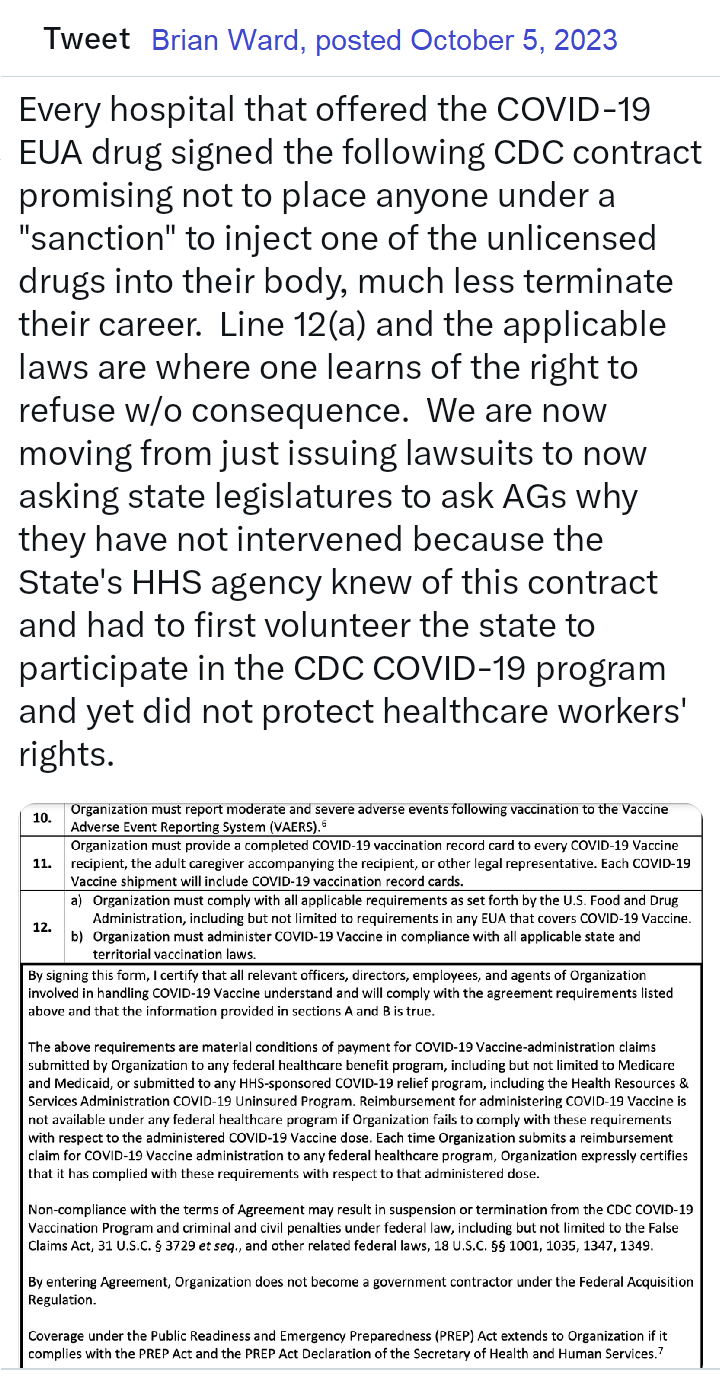 Brian Ward - Twitter Oct 25, 2023 Legal Fact: Any state that penalized citizens or denied unemployment benefits to an individual terminated for the sole reason of refusing to inject an unlicensed investigational drug into their body violated the individual's Fourteenth Amendment Equal Protection and Due Process rights. The U.S. Congress conferred legal authority onto an individual to either accept or refuse an EUA product. Both options were enacted by a valid act of Congress and must be equally protected. Moreover, the Supremacy Clause of the Constitution denied that state authority from interfering in the chosen option. The state established what courts call an Unconstitutional Condition. SCOTUS said: "But the power of the state in that respect is not unlimited; and one of the limitations is that it may not impose conditions which require the relinquishment of constitutional rights. If the state may compel the surrender of one constitutional right as a condition of its favor, it may, in like manner, compel a surrender of all. It is inconceivable that guaranties embedded in the Constitution of the United States may thus be manipulated out of existence." Governors and state agency directors violated their oath of office & the Constitution the moment they required COVID-19 EUA participation and or penalized an individual's federally protected option. They deprived citizens of their interest in liberty and property and, unfortunately for some, their very lives, all without due process. They did so by applying the law unequally demoting those who refused to that of a second-class citizen. Legal Fact: 21 U.S.C. §360bbb-3 and the PREP Act expressly restrict public and private employers from conditioning access to employment and other benefits upon a person injecting an FDA-classified experimental drug (Pfizer-BioNTech COVID-19 Vaccine) into their body. The CDC stated, "Coverage under the Public Readiness and Emergency Preparedness (PREP) Act extends to Organization if it complies with the PREP Act and the PREP Act Declaration of the Secretary of Health and Human Services." "IF IT COMPLIES" is the key phrase here. When a governor issued a proclamation that directly violated the federal statute, the governor did not comply and fraudulently amended the federal law in violation of the Supremacy Clause. The PREP Act and 21 U.S.C. §360bbb-3 provide a legal right to individuals considering participation in the product/activity. That legal right is the option to accept or refuse. Therefore, the immunities provided to persons participating in activities under the PREP Act extend only so far as they do not force persons to participate in the product/activity. Governors, employers, hospitals, all FORCED (under threat of a penalty) individuals to participate in violation of federal law. Force does not have to mean physical force. It can be the force of law, rule, or other means having the same negative effect as physical force. The courts have said that force means to prevent a person or cause a person to participate in an activity outside of their free will and voluntary consent. Significant lawsuits inbound! 12:45 PM · Aug 29, 2023 Brian Ward Aug 2022 BREAKING: LA Superior Court requiring LAPD to reinstate an officer terminated for refusing the vax mandate. Full back pay too! This is under a Writ of Mandamus, which is rare. Legal Fact: "Nothing in this section (EUA Law) provides the [HHS ] Secretary any authority to require any person to carry out any activity that becomes lawful pursuant to an authorization under this section, and no person is required to inform the Secretary that the person will not be carrying out such activity." - The Secretary may grant access to an unlicensed drug (Pfizer-BioNTech COVID-19 Vaccine) during an emergency but he can not mandate that anyone manufacture, distribute, store, administer, or receive the product. His authority is non-transferable, nor may he delegate it to another person. Therefore, by what authority are universities and private employers mandating that which Congress prohibits? EUA drugs are "controlled" drugs by Congress, and no person may participate in them outside of the conditions established by Congress. Moreover, Congress expressly prohibits private employers from interfering with your choice of accepting or refusing participation in the product. It was illegal - It is illegal - and it is being remedied in court. We will not allow this September to be a repeat of years past. 2:18 PM · Aug 21, 2023 Legal Fact: 100% of all hospitals and nearly all universities signed a FEDERAL agreement to abide by the ethical principles of the Belmont Report, though few know it, ANYTIME they involve a human with an investigational medical product such as any available COVID-19 drug. The report is only 10 pages long, but it holds in part: (1) Respect for persons incorporates at least two ethical convictions: first, that individuals should be treated as autonomous agents, and second, that persons with diminished autonomy are entitled to protection. The principle of respect for persons thus divides into two separate moral requirements: the requirement to acknowledge autonomy and the requirement to protect those with diminished autonomy, (2) To show lack of respect for an autonomous agent is to repudiate that person's considered judgments, to deny an individual the freedom to act on those considered judgments, or to withhold information necessary to make a considered judgment, (3) Respect for persons requires that subjects, to the degree that they are capable, be given the opportunity to choose what shall or shall not happen to them. BONUS ROUND - All US States and Territories signed this agreement pre-pandemic too. Yup, no one knows this either, including state attorneys general. Lastly, unlike the Nuremberg Code, the Belmont Report has the force of law via federal statute and contract. Last edited9:28 PM · Aug 2, 2023 Brian Ward via Twitter The VERY first EUA issued was in 2005 for the Anthrax investigational drug for service members and civilian employees of the DoD. The EUA stated: A. Individuals (service members and civilians) who refuse anthrax vaccination will not be punished. (Emphasis added) B. Refusal may not be grounds for any disciplinary action under the Uniform Code of Military Justice. C. Refusal may not be grounds for any adverse personnel action. Nor would either military or civilian personnel be considered non-deployable or processed for separation based on refusal of anthrax vaccination. D. There may be no penalty or loss of entitlement for refusing anthrax vaccination, E. This information shall read in the trifold brochure provided to potential vaccine recipients as follows: You may refuse anthrax vaccination under the EUA, and you will not be punished. No disciplinary action or adverse personnel action will be taken. You will not be processed for separation, and you will still be deployable. There will be no penalty or loss of entitlement for refusing anthrax vaccination. Nothing in law has changed to negate the authority of DoD members to refuse EUA COVID-19 drugs except the 6 civilian appointees engaged in willful misconduct against our Armed Forces. 11:51 PM · Sep 3, 2023  by Rose Rohloff  The 2009 HITECH Act and the Center for Medicare Medicaid Services’ (CMS) Meaningful Use regulations caused a massive spend for electronic medical records (EMRs), the push for interoperability, as the solution to healthcare quality. However, EMRs are not solutions - along with massive IT overhead spend with decreasing quality - because in a high percent of instances, nurses and doctors don’t even read them. A 40-year old mother went to the doctor after treating herself holistically for some laryngitis, stuffy nose, congested sinus, with continued symptoms after five days. After an exam, the doctor stated, “I am not going to give you antibiotics. You do not have a fever; your lungs sound clear. It looks like a little virus with severe allergies. I recommend an antihistamine.” The patient told him, “Thank you for not putting me on antibiotics when they are not needed, that makes me happy.” He responded, “I am glad you are glad.” He then said something and the patient responded, “I have MS.” He responded, “Oh wait, you have Multiple Sclerosis?” This story is sadly too often the new normal, numerous instances of patients and their caregivers stating issues of diagnosing with medication prescription, or misdiagnosis; the doctor or nurse having no idea of pre-existing conditions or a full list of medications currently being taken, a lack of care coordination or care planning because the time was not taken to simply read the chart (whether written or electronic), and ensuring a comprehensive history followed by the necessary physical assessment. No physician or nurse should walk in to care for a patient without first having read the patient’s record, knowing all current information, the last visit/healthcare encounter, chronic conditions/comorbidities, and all medications; then, asking for updates of changes. Unfortunately, even without having to decipher poor handwriting, being able to read clean typed text, clinicians are not simply reading the basics of information they should before doing any diagnosis, planning and care, or prescribing of medications. 
There are pitfalls with IVF that are not discussed. And, this business end of reproduction is more often than not cash only. There are virtually ZERO long term studies regarding what effect-impact freezing, and a host of other ‘things’, that are done to the egg, or sperm, or the embryos that have (or could have) on the child that is produced. This 'miracle of modern medicine' could be good ... or just OK ... or it could be very, very bad. Science has rubbed the lamp and we cannot put the genie back in the bottle. After counseling many women in my career, the great emotional toil let alone the finances are not discussed. The ethical check is also missing regarding instances of doctors using their own sperm such as the Indiana doctor who in 2016 used his own sperm at least 50 times. As the character Dr. Ian Malcom (played by Jeff Goldblum) said in the 1993 movie Jurassic Park, “Your scientists were so preoccupied with whether they could (create life) that they didn’t stop to think if they should.” by Karen F., (Ret) RN, NP OB & Palliative Care  by Rose Rohloff
As a 35-year healthcare veteran, I am a firm believer of cross-pollinating successful processes from other industries into the healthcare industry, for positive transformation. Delivering quality care will continue to be complex and challenging, with the need to leverage solutions that work. And SEAL teams are a proven efficient and effective success in the military. By rebranding PC teams and the team process, expanding with additional SEAL successful methods and approaches, we can create the Healthcare version of SEALs (sea, air, land), as APAC Teams (acute, post-acute, and community) - expanding the process to operate in every environment versus only in facilities, for enhancing the quality of care of high risk patients versus limiting to end-of-life cases. The following chart displays characteristics of SEALs, obtained from several former SEAL, special operation personnel, and military officers; with several of the attributes emulating characteristics regarding the successful palliative care (PC) team process.
* https://www.navy.com/dam/Navy/Navy-IMG/Downloads/pdf/enlisted/seal-brochure.pdf ** http://www.nsonswmentor.com/Navy-SEAL.html Within the industry, PC is still aligned or mistaken with hospice, as demonstrated in the following two scenarios. Recently, a viral video was circulated and applauded, Australian paramedics fulfill dying woman’s wish to go to the beach, telling the story of a Hervey Bay crew transporting a patient to the palliative care unit, but she wished she could, “Just be at the beach” instead, and so the crew drove to the beach to provide her peace, based on her wishes of quality of life. This story is lovely regarding true care of a patient. Additionally, in April of this year I attended the Becker’s Hospital Conference in Chicago with the top leaders in healthcare, with a wonderful presentation about business analytics regarding palliative care, end-of-life. Both stories demonstrate clearly that palliative care is still being confused with hospice, or limited to a specific unit definition, instead of the effective use of the team process use with complex and/or chronic conditions.
However, what is it continuing to do to their brains having more medications and anesthesia, while it may not be improving their actual quality of life?” With APAC team coverage, a non-end-of-life case can be reviewed with a sound plan of care based on the desired quality of life for the patient and family. The PC coverage in the community has been focused on cancer patients, with a high focus on children. With the demonstrated cost savings and positive outcomes with The value of palliative care teams (HFMA, March 2013), the community coverage can be successful for individuals with multiple comorbidities, such as diabetes with congestion heart failure and hypertension; as well as elderly who are being targeted when ‘sundowning’ with fraud scams, or confused with medication regime, and those with family living in other states who are their primary support system/durable power of attorney. It is daunting, emotionally and financially, for the families of high-risk consumers to search out the various interdisciplinary resources such as dieticians, social workers, case managers, pharmacists, nurse practitioners, and spiritual counselors. APAC teams would also address the necessary information gathering for determining the real issues of consumers, for example, who needs dietary changes or removal of drugs with side effects before being prescribed new medications by physicians, causing even more side effects or noncompliance, and self medicating or opiate abuse. PC teams can be expanded to APAC teams utilizing the successful palliative care process across the care and health continuum, eliminating the end-of-life association, and differentiating from the terminally ill care of hospice. Just as SEALs operate in every environment (air, sea and land), APAC teams can be an extension of PC teams to be the quick, nimble action teams in all settings, especially the community, for patients with complex and chronic conditions.  by Rose Rohloff  Sleep apnea affects about 18 million people. This condition is linked as a major contributor to atrial fibrillation as well as multiple other health issues. Individuals have previously had to go to sleep centers for diagnosis, which is time consuming, and people generally do not sleep well in a foreign environment. "The Mayo Foundation for Medical Education and Research (Mayo Clinic) has purchased the WatchPAT device, an FDA-approved sleep apnea home testing device developed by Israeli medical diagnostics company Itamar Medica." nocamels -- Israeli innovation News WatchPAT is an FDA-approved portable diagnostic device that uniquely uses finger based physiology and innovative technology to enable simple and accurate Obstructive Sleep Apnea (OSA) testing while avoiding the complexity and discomfort associated with traditional air-flow based systems. 
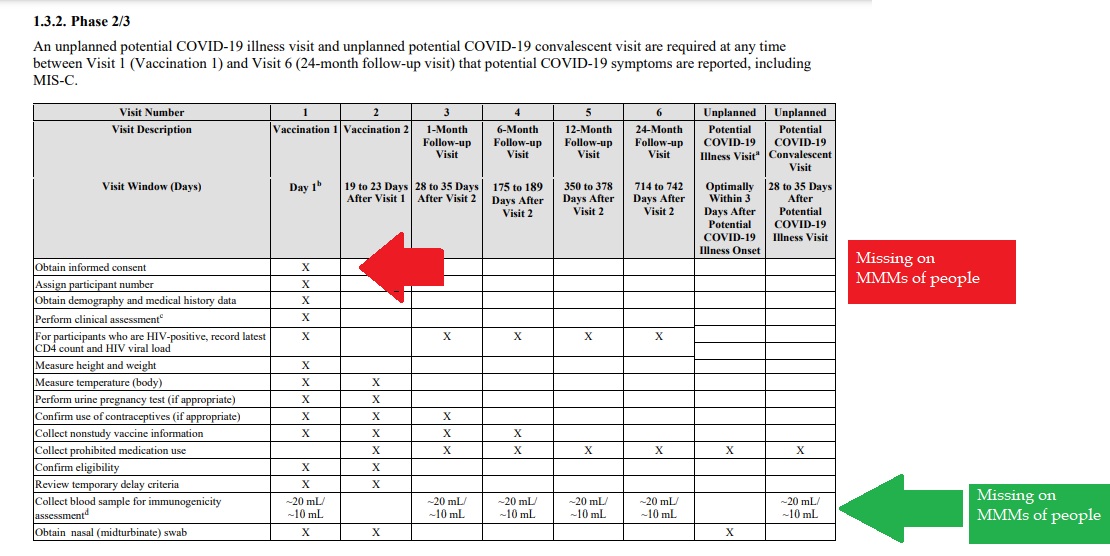
The lab model has great benefit, and feasible when costs are not prohibitive, especially avoiding a doctor's office visit when only ordering labs, or if one wishes to bring any abnormal readings then to the doctor's attention. With the many lessons learned from an aborted (shady) startup, marketed to disrupt the healthcare industry with its counterfeit technology, the direction for having consumer-driven as the process should not be overlooked - and actually be revisited to expand upon the great health ownership model of good disruption to healthcare.  The healthcare industry has used perioperative morbidity and mortality reviews (M&Ms) for blunt evaluations, to continuously improve the understanding of and performance in surgical intervention. Since the industry touts Population Health and Patient Engagement as top initiatives, health systems can use the successful process of M&Ms to perform Population Health and Patient Engagement reviews (P&Ps) of individual cases, for ensuring quality care processes. [read more] Published Becker's Hospital Review.  |
||||||||||||||||||||||||||||||||||||||||||||