Compiled Rose Rohloff from input by Dr. Peter McCullough and Dr. James ThorpMany persons may have been illegally coerced into taking the Covid shots.(see blog entry regarding the 1974 National Research Act) The following is an extensive Spike Protein (SP-C) lab panel, sectioned into subpanels (a panel is a collection of several lab tests), for evaluating if you systems may have been impacted by the spike proteins - with or without existing symptoms. Note some individual labs may be duplicated in various panels and will not have to be duplicated. Champion your own care and consult with your choice of physician with informed consent. General Tests and Evaluation of Cardiac
The following evaluate antibody (Ab) in your blood, proteins made by the immune system to fight foreign bodies (bacteria, virus …)]**
For women of reproduction age
For autoimmune and/or bleeding issues
 1No commercially available test for circulating spike amounts are available at this time and will update as one becomes available. Serum Spike Antibody (Ab) is the surrogate at this time. Higher spike Ab titer correlates with severity of infection/long COVID. Pathologists are able to determine if tissue spike is from Shots/Injections versus infection via correctly performed autopsy, as per Dr. Ryan Cole in deposition of case. “Normal” Value-ranges & Description of various testsSome parameters vary slightly based on which lab is used - low or high readings should be determined by the specific lab being used at the time of lab test, and for individuals regarding their baselines, underlying conditions.  D-dimer CBC CRP CMP Various Antibody testing to determine if your immune system is or is not fighting off a foreign substance. TSH: ***
Amenorrhoea Panel

0 Comments
"Ninth Circuit Court Full Details... read each bullet point baby! (1) The court ruled that the district court misapplied the 1905 Jacobson case because LAUSD relies on a drug that Plaintiffs plausibly alleged did not prevent the spread of the virus. (2) LAUSD has changed its mind about requiring the vaccine and therefore, the case cannot be mooted because LAUSD has proven it will just enact it again later. (3) The court said, "But even if the materials offered by LAUSD are subject to judicial notice, they do not support rejecting Plaintiffs’ allegations. LAUSD only provides a CDC publication that says “COVID-19 vaccines are safe and effective.” But safe and effective for what? LAUSD implies that it is for preventing transmission of COVID-19 but does not adduce judicially noticeable facts that prove this." (4) "Pursuant to more recent Supreme Court authority, compulsory treatment for the health benefit of the person treated—as opposed to compulsory treatment for the health benefit of others— implicates the fundamental right to refuse medical treatment. Plaintiffs’ allegations here are sufficient to invoke that fundamental right. Defendants note that the vaccination mandate was imposed merely as a “condition of employment,” but that does not suffice to justify the district court’s application of rational-basis scrutiny." (5) MUST READ THIS..."In Washington v. Glucksberg, 521 U.S. 702 (1997), the Court explained that Cruzan’s posited “‘right of a competent individual to refuse medical treatment’” was “entirely consistent with this Nation’s history and constitutional traditions,” in light of “the common-law rule that forced medication was a battery, and the long legal tradition protecting the decision to refuse unwanted medical treatment.” Id. at 724–25 (citation omitted). Given these statements in Glucksberg, the right described there satisfies the history-based standards that the Court applies for recognizing “fundamental rights that are not mentioned anywhere in the Constitution.” Dobbs v. Jackson Women’s Health Org., 597 U.S. 215, 237–38 (2022). The Supreme Court’s caselaw thus clarifies that compulsory treatment for the health benefit of the person treated—as opposed to compulsory treatment for the health benefit of others— implicates the fundamental right to refuse medical treatment." https://cdn.ca9.uscourts.gov/datastore/opinions/2024/06/07/22-55908.pdf… Who is in charge of healthcare? Is your Health insurance coverage invalidated/exempt? 5G and edc4/12/2024 by Rose RohloffEach individual should be in charge of their own healthcare decisions, safety surroundings, and be treated individually. So, a good question to ask, "Who actually is in charge?" Laws and Executive Orders (EOs) regarding healthcare under "public health"Created by Todd Calendar, Esquire H.R.3832 - Disease X Act of 2023 118th Congress (2023-2024) Open "disease" cart blanc for them to choose (or orchestrate?) ‘World Health Organization (WHO) Has No Authority to Dictate U.S. Health Policy’ factcheck.org March 2, 2023 "Although the accord is being called ... a treaty or another kind of binding agreement, such as the WHO Framework Convention on Tobacco Control, or a nonbinding agreement, such as the Paris Climate Accord. “As with all international instruments, any accord, if and when agreed, would be determined by governments themselves, who would take any action while considering their own national laws and regulations,” a WHO spokesperson told us." Federal and Local Governments would be in charge regarding any Rights violations. The accord is accumulation of monies $$$ to be "distributed" to various countries/persons, in the name of public health.
LTC (ret) Green Beret, Doc Pete Chambers, MD, bioweapons expertRisk of 5G rolled out, without safety studies, by Federal, State and Local governance. Communities were not asked regarding rollout, or informed regarding safety issues of 5G. Are we experiencing history repeating the dangers of DDT, Asbestos, many FDA "approved" drugs recalled because they lacked safety, etc.?
Are individual healthcare insurance policies, the underwriters of policies, being invalidated without the knowledge of people, and against their choice - through lack of knowledge, lack of informed consent, and through illegal coercion? Electromagnetic Radiation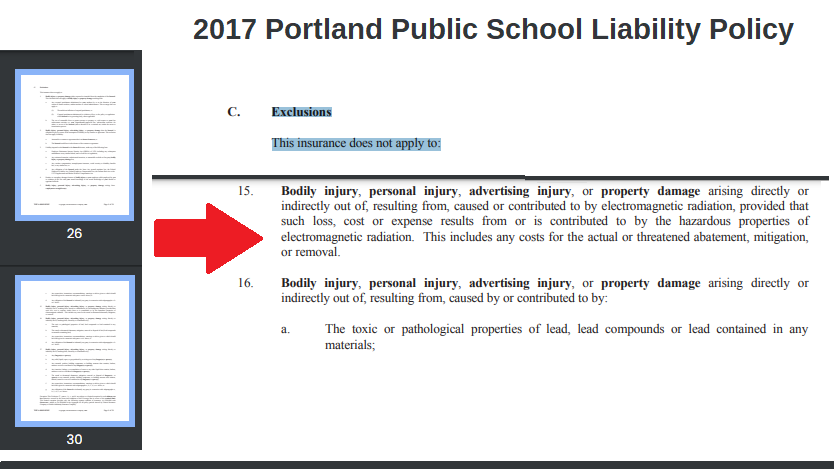 Public School Healthcare Policy - page 30 - under Exemption section starting page 26. 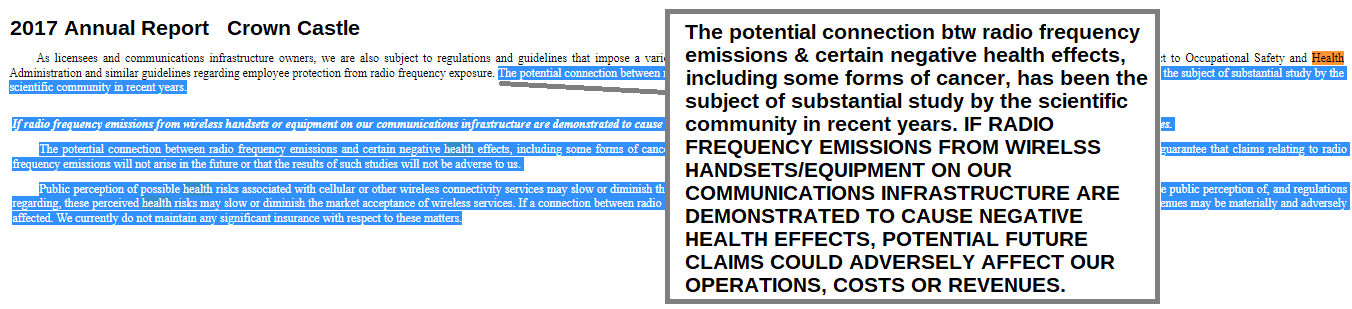 2017 Annual Report Crown Castle 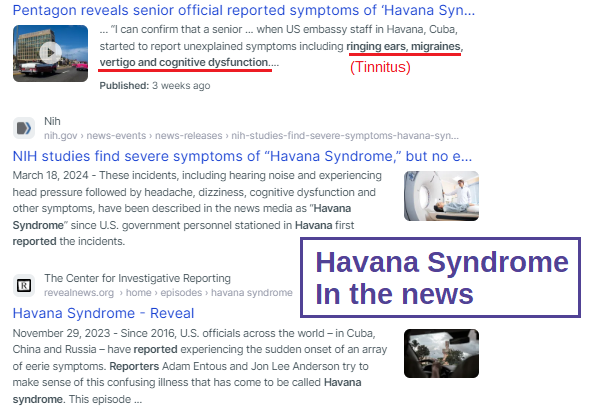 Havana Syndrome suddenly "in the news" Endocrine Disrupting Chemicals (EDCs)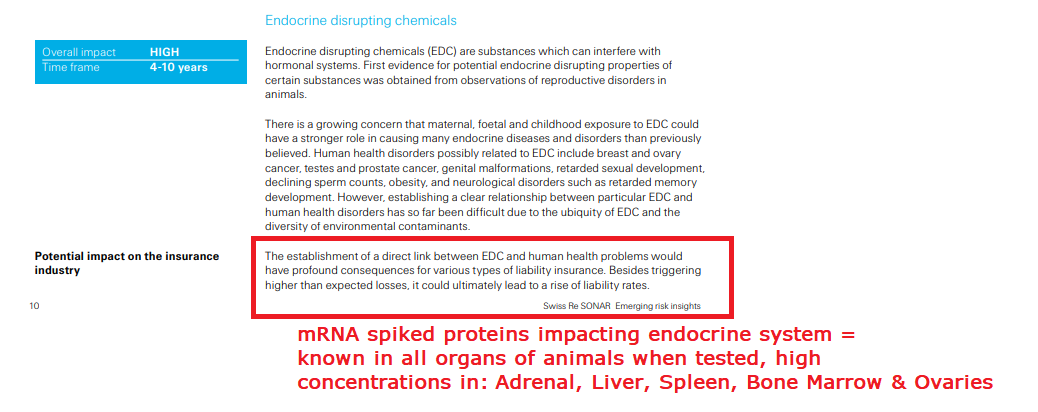 Major underwriter for insurance, exemption for Endocrine disrupting chemicals (EDCs)  Pfizer document - animal testing, spike protein to all organs including endocrine system by Numerous expertsMy desire is to provide several articles from those adroit in the subject. COPPER: the less talked about, and important trace mineral, the importance of Zinc, and when taking high Zinc, make sure you know the ratio of zinc to copper supplements.
Ralph Baric and other scientists knew in 2010 the "antidote"/treatments for the upcoming virus(es). He coauthored the discovery "Increasing the intracellular Zn(2+) concentration with zinc-ionophores like pyrithione (PT) can efficiently impair the replication of a variety of RNA viruses". Dr. Vladimir Zelenko based his effective protocol after watching the "MedCram Lecture 34 by Dr. Roger Seheult about the use of zinc and zinc ionophores. Zinc is an essential mineral for humans, and a little extra zinc is sometimes used to lessen the intensity of colds and sore throats. An ionophore is a chemical that opens the cell wall to allow minerals (ions) to enter. ‘First do no harm’ Zinc is an over-the-counter supplement. Hydroxychloroquine (HCQ) is a reliable ionophore, and it has a well-established dosing regimen and safety profile." Zinc ionophores "increase the intracellular concentration of Zinc ions causing significant biological effects. Review ionophores: HCQ, EGCG (a plant compound particularly prominent in green tea) and Quercetin (particularly in citrus fruits, apples, onions, parsley, sage, tea, and red wine. Olive oil, grapes, dark cherries, and dark berries such as blueberries, blackberries, and bilberries are also high in quercetin and other flavonoids.) "
Mount Sinai "Copper is a mineral that is found throughout the body. It helps your body make red blood cells and keeps nerve cells and your immune system healthy. It also helps form collagen, a key part of bones and connective tissue. Copper may also act as an antioxidant, reducing free radicals that can damage cells and DNA. Copper helps the body absorb iron. Your body also needs copper to make energy."
Dr. Shiva The Power of Copper to fight virus, bacteria on contact
Copper has even been shown to be very effective at exterminating the much-dreaded hospital ‘superbug’ MRSA. In tests sponsored by the Copper Development Association, a grouping of 100 million MSRA bacteria atrophied and died in a just 90 minutes, when placed on a copper surface at room temperature. The same study found that the same number of MSRA bacteria on both steel and aluminium surfaces actually increased over time. On looking at these figures, many scientists have concluded that the installation of copper-based fixtures such as taps, light switches, door handles, door knobs, pull handles, and push plates in areas such as hospitals could save thousands of lives each year. Professor Bill Keevil, head of the microbiology group at Southampton University, added his voice to the growing scientific consensus behind this by advocating the use of Copper and Brass door furniture, fixtures and fittings in public places and on public transport, as they could dramatically cut the threat posed by superbugs. In research published in the journal Molecular Genetics of Bacteria Professor Keevil wrote: “There are a lot of bugs on our hands that we are spreading around by touching surfaces. In a public building or mass transport, surfaces cannot be cleaned for long periods of time… Until relatively recently brass was a relatively commonly used surface. On stainless steel surfaces these bacteria can survive for weeks, but on copper surfaces they die within minutes… We live in this new world of stainless steel and plastic, but perhaps we should go back to using brass more instead.” In addition to direct contact killing of bacteria and harmful microbes, amazingly Copper surfaces have been found to exude an antimicrobial 'halo' effect on surrounding non-copper surfaces. Research in the intensive care unit a Hospital in Greece found that other surfaces up to 50 centimetres from copper surfaces experienced 70% microbial reduction, compared to the same surfaces with no proximity to copper-based materials. The ‘Halo’ effect was also observed in trials at a U.S. clinic in 2010. This amazing effect demonstrates just how powerful copper is as a weapon against bacteria." www.morehandles.co.uk  Videos to listen toThe latest simple, easy-to-follow overview of the paper trail showing crimes against humanity, and how a few of the many are now complicit with failure to act on the crimes,  Easy-to-follow overview of the paper trail showing crimes against humanity American Biological Threat Consultant at the European Parliament in Strasbourg, France on September 13/2023 https://rumble.com/v3sahot-dr-david-e-martin-who.html Coronavirus Gain-of-Function Research at the Covid Summit in Brussels, Belgium May 2023 https://rumble.com/v2mwrgm--dr.-david-martin-documenting-coronavirus-gain-of-function-research-at-the-.html Dr. Martin is impressive with his work, and how he articulates things https://twitter.com/i/status/1615707500946546689 Martin was the first to stipulate Pharma with DoD, CIA 7-12 minutes great breakdown of science that it is not about virus, protein fragment! 13 minutes Insert mRNA fragment, so cell makes Spike Protein. 17 minutes Acts of Terror 18 minutes AntiTrust laws violated, conspiracy 20 minutes Interlocking Directorates, Sherman Act 22 minutes Civil law, used by Trade Commission - cannot do deceptive marketing 27 minutes unlawful lack of informed consent Institutional Review Board never created, even in the case of emergency Code 21CFR section 50.24   by Rose Rohloff
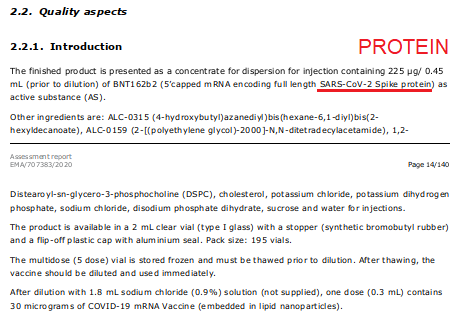
 Exhibit A: EcoHealth Alliance proposal to DARPA page 3; intention = GOF as per DARPA  Exhibit B: Pfizer document components of the shots 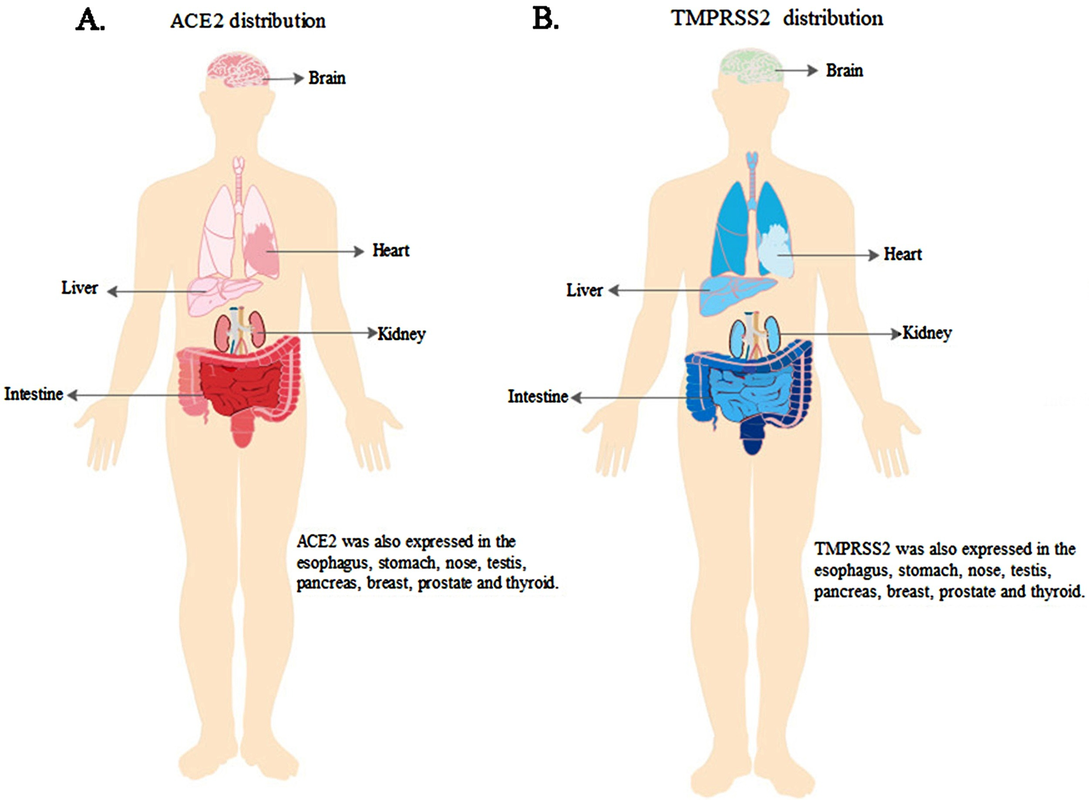 Exhibit C: ScienceDirect "ACE2, TMPRSS2 distribution and extrapulmonary organ injury in patients with COVID-19" Nov 2020 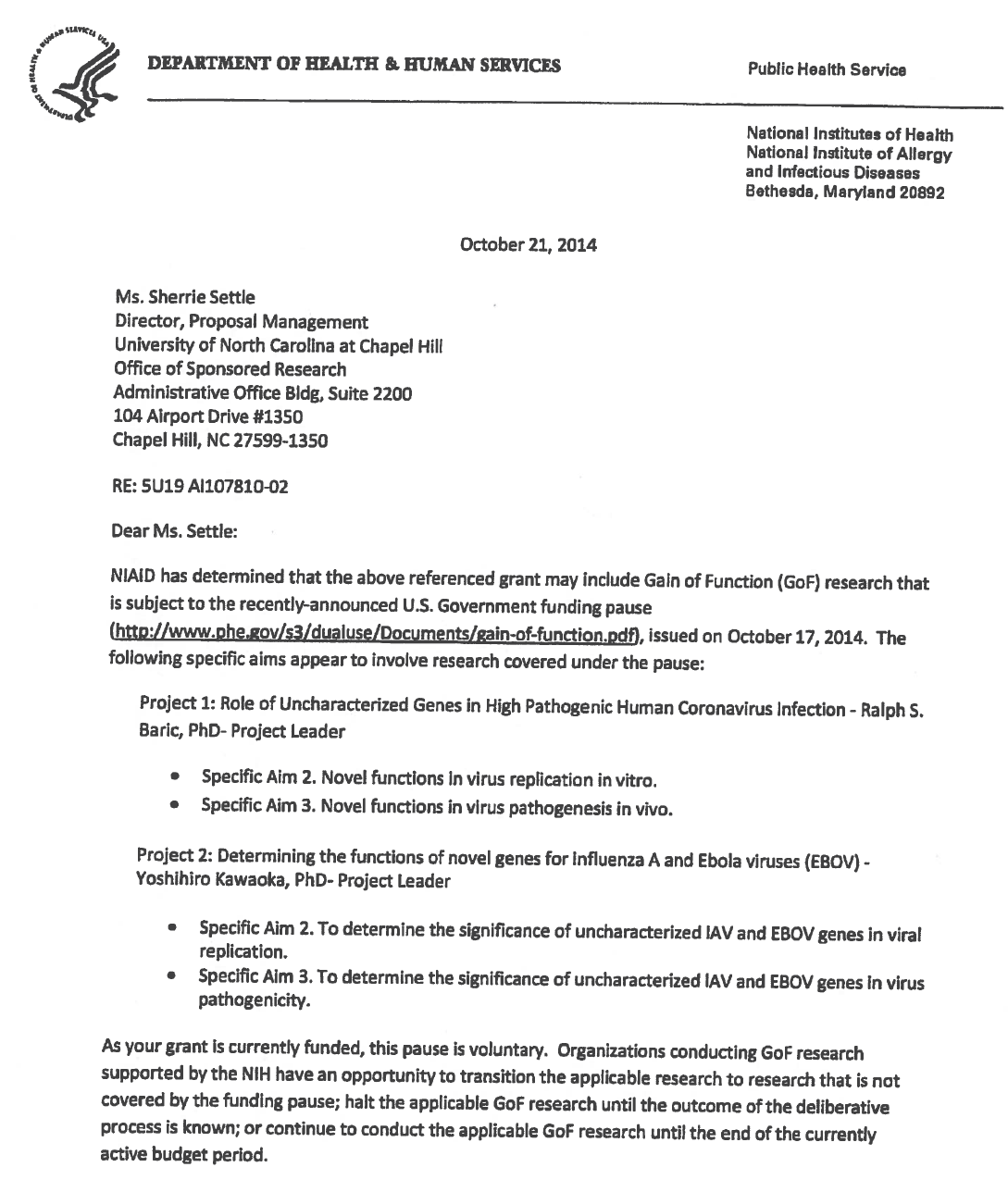 Exhibit D: Un of NC letter GOF * Date: written 2015 posted 2016 * Not natural: chimeric infectious clones, GOF  Exhibit E: Baric, Univ NC, Chapel Hill - 2016
The 1974 Research Act was created in entirety from the Belmont report, and put into place to prevent the Government, it agencies or representatives, military and private companies, from violating an individual's freedom: by forcing, tricking or coercing persons for research, testing and administration of unknown injections/materials, and experimental procedures. This law was enacted after a century long track record of precedence including, and not limited to, the following:
Demonstrated lack of Respect for Persons and their protections in violation of 1974 law. 1- Autonomous agents, individuals capable of deliberation about personal goals and of acting under the direction of such deliberation. The Government and companies have to give weight to autonomous persons' considered opinions and choices, and cannot obstruct their actions and judgments, nor deny individual freedom to act on considered judgments, and cannot withhold information necessary to make a considered judgment. Necessary information includes - but not limited to - all medical opinions by established, industry experts, health status, the necessary assessments, labs, with close monitoring of physical lab and test follow ups of each and every autonomous persons as part of clinical research and testing, along with full documentation of testing, efficacy, use of chimera for research and testing, any and all conceivable side effects, and interactions of conditions.
 2- persons with diminished autonomy are entitled to added protections. Violators to the law have been marketing to the most vulnerable, including the immature and the incapacitated who were in need of extra, added protections, even to the point of excluding them from any injections or procedures which may harm them; violating added safety precautions for children, elderly, or those with diminished capacity. Informed consent - must include full disclosure of ALL contents to be injected, any and ALL possible side effects (which can be several pages long), how those persons are individually to be closely monitored, safety guidelines, and above all the right to say no before or at any time, and full reporting of all individuals regarding their safety monitoring/labs/assessments, and any and all side effects. By promoting COVID shots all still under clinical trial/research, and coercing with careers/jobs, inability to travel, etc. in order to take the shots, this law is being violated through: lack of informed consent, lack of protections of autonomous persons, and/or illegally acting as IRB safety board members marketing to those not autonomous and capable of self-determination, with higher standards of protection to be invoked, and assuming the role for their safety. The maxim "do no harm" has long been a fundamental principle of medical ethics. Claude Bernard extended it to the realm of research, saying that one should not injure one person regardless of the benefits that might come to others. An agreement to participate in research constitutes a valid consent only if voluntarily given. This element of informed consent requires conditions free of coercion and undue influence. Undue influence also includes offers of an excessive, unwarranted, inappropriate or improper reward or other overture in order to obtain compliance. Also, inducements that would ordinarily be acceptable may become undue influences if the subject is especially vulnerable as in the case of targeting children, persons with limited capacity, and elderly with elements of mental defect, or instilling fear. Short term morbidity and mortality cases from the shots are well reported and known, such as death, myocarditis along with spontaneous cardiac arrest with no warning, debilitating neurological conditions, etc. And, there is no means yet to determine mid and long term effects because Phase I trials have not been competed, let alone Phase II and III - which is vital information in order to determine informed consent. Injustice has been performed with companies and government representatives, by involving vulnerable subjects, including the young, those unable to fully comprehend with all necessary information, and scaring parents with compromised capacity for free consent. In addition to lack of individual, tightly scheduled, continual monitoring and follow ups, autopsies of all persons involved in this trial participation should be conducted for reporting by the pharmaceuticals companies for any and all persons who received the shots, as well as labs determining efficacy and detriments (as examples, antigen creation, D-dimer, Pulse Cardiac and Troponin Tests) for all those who were coerced or unduly influenced to participate in research. This law was created to protect people from government abuse through experimentation. The government cannot arbitrarily dismiss components, create resolutions or stipulations to supersede the law, as to invalidate its protection of individuals from them, including, but not limited to Health and Human Services (HHS) Center for Disease Control (CDC), Food and Drug Administration (FDA), National Institute for Health (NIH), etc. and pharmaceutical companies, etc. Persons have been illegally acting as members of, or bypassing, IRB safety review and monitoring of each and every person receiving injections, with open undue influence and coercion, to participate in Covid injections. Coercion has been especially directed to the diminished autonomous, children and elderly, through TV ads, library recordings, verbal encouragement, schools or other public venues acting as government agents, and/or clinical researcher recruiting participants, and/or illegally as untrained IRB member who is not following up to ensure safety of the people they recruited, coerced or used undue influence. Overall lack of informed consent has become too often common practice across the healthcare industry, including people being given consent forms hours or minutes prior to surgery; no alternative treatments or lifestyle-nutrition changes prior to medications begin prescribed, and undue influence to intubate or perform surgery on patients in lieu of alternative treatments.
Lawsuits for unconstitutional violation of laws regarding shotsPosted by Brian Ward on Twitter Guess what? Defendants in our lawsuits no longer argue that they had a right to mandate EUA drugs due to their state's at-will employment doctrine. That the EUA drugs can be mandated. That they had the authority to even issue the mandate. Why? Read the 127 pages, and then you'll understand that it was a legal lie from the beginning, but due to the novelty of the laws, no one knew of them. As courts have stated, "sometimes laws take naps," and these laws never showed up for work until now. https://coloradomedicalfreedom.com/wp-content/uploads/2023/08/Stamped-Final-Complaint.pdf full document https://coloradomedicalfreedom.com/wp-content/uploads/2023/08/Stamped-Final-Complaint.pdf page 127 C. the Secretary has no “authority to require any person to carry out any activity that becomes lawful pursuant to an authorization under this section…” 549. In 2005 Congress passed the PREP Act94 which provided the following regarding preemption of state law: (8) During the effective period of a declaration under subsection (b)…no State or political subdivision of a State may establish, enforce, or continue in effect with respect to a covered countermeasure any provision of law or legal requirement that— (A) is different from, or is in conflict with, any requirement applicable under this section; and (B) relates to the…administration…of the covered countermeasure, or to any matter included in a requirement applicable to the covered countermeasure under this section or any other provision of this chapter, or under the Federal Food, Drug, and Cosmetic Act [21 U.S.C. 301 et seq.]. 550. Therefore, via the PREP Act and 21 U.S.C. §360bbb-3, Congress expressly prohibits Defendants from: A. interfering with the authority of the Secretary, B. establishing a condition not authorized by the Secretary, C. establish conditions contrary to the Secretary and the congressional statute under 21 U.S.C. §360bbb-3, D. mandate participation in any 21 U.S.C. §360bbb-3 product or PREP Act activity, E. interfere with an individual considering participation in a 21 U.S.C. §360bbb-3 product or PREP Act activity, F. penalize a person refusing to participate in a PREP Act product or activity or 21 U.S.C. §360bbb-3 product. 551. The executive branch of the United States Government purchased all COVID-19 licensed and EUA drugs using federal funds. Congress expressly prohibits the federal government Brian Ward @GodsRiddles Nov 1, 2023 Breaking…Gov Gavin Newsom and Kaiser have been sued in federal court for requiring healthcare workers to inject an experimental drug into their bodies as a condition to sell their labors in the marketplace. The requirement violated the workers’ Equal Protection of Laws and Due Process rights. Moreover, Kaiser signed a contract with the CDC promising not to mandate participation but did so anyway. Kaiser and Newsom fraudulently concealed the fact that nurses would be required to forfeit litigation rights if they incurred an injury from the use of the experimental drug. The California Nurses union stood by and refused to stop Newsom’s tyranny, leaving members without representation. Governor Newsom perpetuated the greatest assault on the US Constitution in the state’s history and the CA AG did nothing to prevent it. Worse yet, is that CA and Kaiser already had an agreement with HHS promising to never place an individual under a sanction for refusing to inject federally funded experimental drugs into the body. Legal Fact: medical providers have dual roles in relation to their employees. An employee can be a patient and an employee. Should a hospital mandate the use of a drug under the PREP Act as a condition of employment and the patient is injured then the patient would find it difficult to sue the medical provider for that injury. However, the employee has the right to seek compensation irrespective of the PREP Act because it’s an on the job injury. Of course this opinion does not account for the laws of all 50 states but demonstrates why one should seek legal advice immediately upon sustaining an injury. This is not my opinion but the chief judge of the 11th circuit who wrote a slip opinion when he was AL AG denoting the company is liable for vaccine injuries because the company believes the vaccine would benefit the company. Last edited10:55 AM · Nov 10, 2023
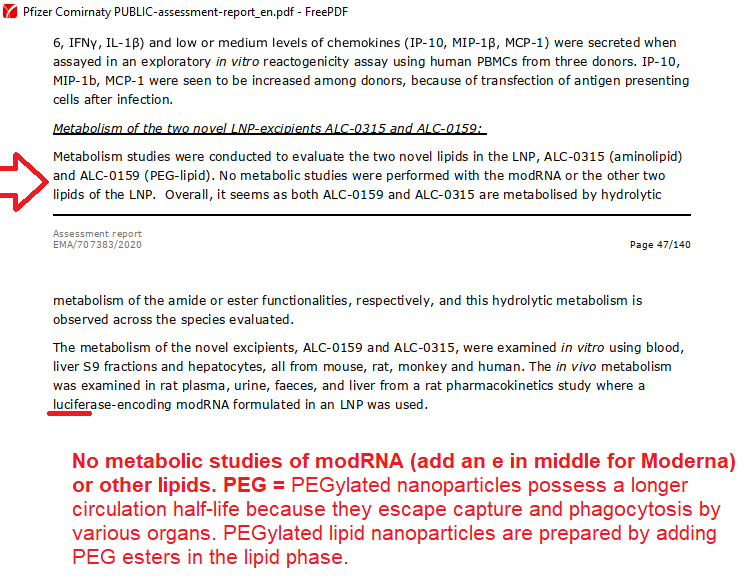
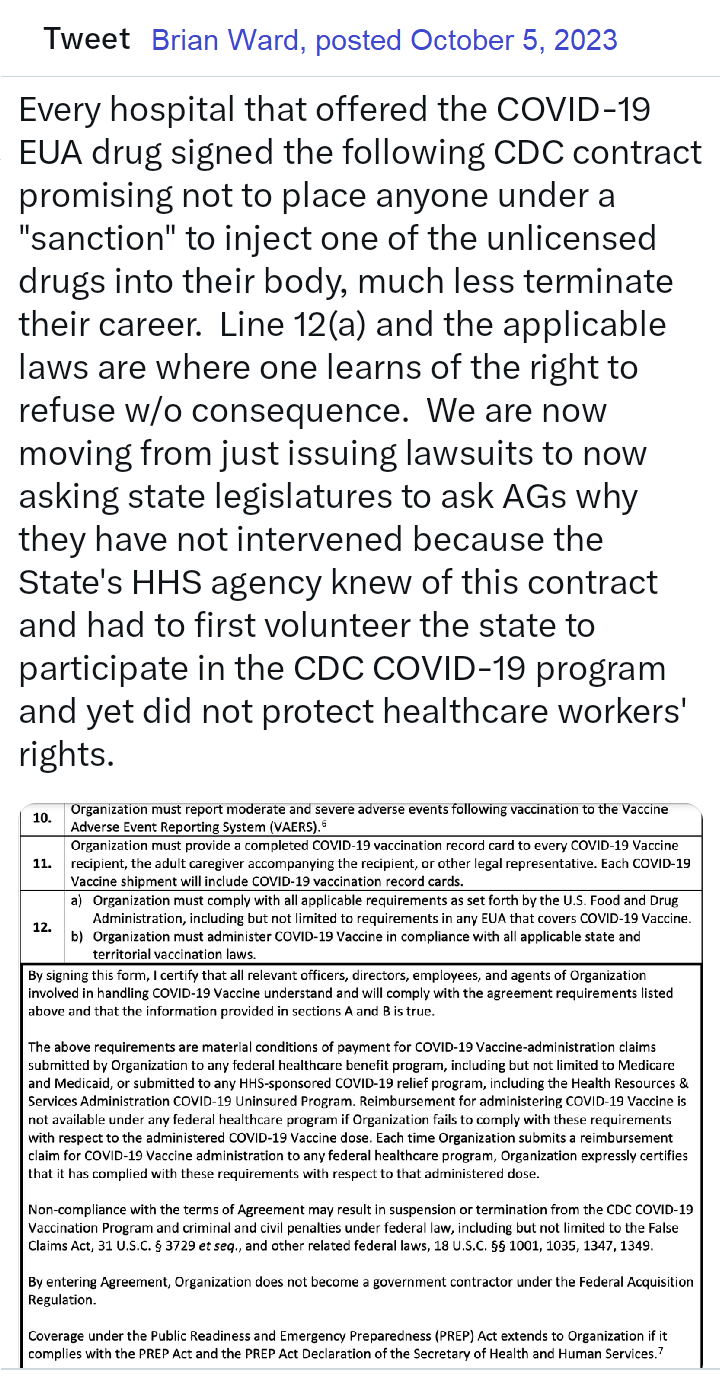 Brian Ward - Twitter Oct 25, 2023 Legal Fact: Any state that penalized citizens or denied unemployment benefits to an individual terminated for the sole reason of refusing to inject an unlicensed investigational drug into their body violated the individual's Fourteenth Amendment Equal Protection and Due Process rights. The U.S. Congress conferred legal authority onto an individual to either accept or refuse an EUA product. Both options were enacted by a valid act of Congress and must be equally protected. Moreover, the Supremacy Clause of the Constitution denied that state authority from interfering in the chosen option. The state established what courts call an Unconstitutional Condition. SCOTUS said: "But the power of the state in that respect is not unlimited; and one of the limitations is that it may not impose conditions which require the relinquishment of constitutional rights. If the state may compel the surrender of one constitutional right as a condition of its favor, it may, in like manner, compel a surrender of all. It is inconceivable that guaranties embedded in the Constitution of the United States may thus be manipulated out of existence." Governors and state agency directors violated their oath of office & the Constitution the moment they required COVID-19 EUA participation and or penalized an individual's federally protected option. They deprived citizens of their interest in liberty and property and, unfortunately for some, their very lives, all without due process. They did so by applying the law unequally demoting those who refused to that of a second-class citizen. Legal Fact: 21 U.S.C. §360bbb-3 and the PREP Act expressly restrict public and private employers from conditioning access to employment and other benefits upon a person injecting an FDA-classified experimental drug (Pfizer-BioNTech COVID-19 Vaccine) into their body. The CDC stated, "Coverage under the Public Readiness and Emergency Preparedness (PREP) Act extends to Organization if it complies with the PREP Act and the PREP Act Declaration of the Secretary of Health and Human Services." "IF IT COMPLIES" is the key phrase here. When a governor issued a proclamation that directly violated the federal statute, the governor did not comply and fraudulently amended the federal law in violation of the Supremacy Clause. The PREP Act and 21 U.S.C. §360bbb-3 provide a legal right to individuals considering participation in the product/activity. That legal right is the option to accept or refuse. Therefore, the immunities provided to persons participating in activities under the PREP Act extend only so far as they do not force persons to participate in the product/activity. Governors, employers, hospitals, all FORCED (under threat of a penalty) individuals to participate in violation of federal law. Force does not have to mean physical force. It can be the force of law, rule, or other means having the same negative effect as physical force. The courts have said that force means to prevent a person or cause a person to participate in an activity outside of their free will and voluntary consent. Significant lawsuits inbound! 12:45 PM · Aug 29, 2023 Brian Ward Aug 2022 BREAKING: LA Superior Court requiring LAPD to reinstate an officer terminated for refusing the vax mandate. Full back pay too! This is under a Writ of Mandamus, which is rare. Legal Fact: "Nothing in this section (EUA Law) provides the [HHS ] Secretary any authority to require any person to carry out any activity that becomes lawful pursuant to an authorization under this section, and no person is required to inform the Secretary that the person will not be carrying out such activity." - The Secretary may grant access to an unlicensed drug (Pfizer-BioNTech COVID-19 Vaccine) during an emergency but he can not mandate that anyone manufacture, distribute, store, administer, or receive the product. His authority is non-transferable, nor may he delegate it to another person. Therefore, by what authority are universities and private employers mandating that which Congress prohibits? EUA drugs are "controlled" drugs by Congress, and no person may participate in them outside of the conditions established by Congress. Moreover, Congress expressly prohibits private employers from interfering with your choice of accepting or refusing participation in the product. It was illegal - It is illegal - and it is being remedied in court. We will not allow this September to be a repeat of years past. 2:18 PM · Aug 21, 2023 Legal Fact: 100% of all hospitals and nearly all universities signed a FEDERAL agreement to abide by the ethical principles of the Belmont Report, though few know it, ANYTIME they involve a human with an investigational medical product such as any available COVID-19 drug. The report is only 10 pages long, but it holds in part: (1) Respect for persons incorporates at least two ethical convictions: first, that individuals should be treated as autonomous agents, and second, that persons with diminished autonomy are entitled to protection. The principle of respect for persons thus divides into two separate moral requirements: the requirement to acknowledge autonomy and the requirement to protect those with diminished autonomy, (2) To show lack of respect for an autonomous agent is to repudiate that person's considered judgments, to deny an individual the freedom to act on those considered judgments, or to withhold information necessary to make a considered judgment, (3) Respect for persons requires that subjects, to the degree that they are capable, be given the opportunity to choose what shall or shall not happen to them. BONUS ROUND - All US States and Territories signed this agreement pre-pandemic too. Yup, no one knows this either, including state attorneys general. Lastly, unlike the Nuremberg Code, the Belmont Report has the force of law via federal statute and contract. Last edited9:28 PM · Aug 2, 2023 Brian Ward via Twitter The VERY first EUA issued was in 2005 for the Anthrax investigational drug for service members and civilian employees of the DoD. The EUA stated: A. Individuals (service members and civilians) who refuse anthrax vaccination will not be punished. (Emphasis added) B. Refusal may not be grounds for any disciplinary action under the Uniform Code of Military Justice. C. Refusal may not be grounds for any adverse personnel action. Nor would either military or civilian personnel be considered non-deployable or processed for separation based on refusal of anthrax vaccination. D. There may be no penalty or loss of entitlement for refusing anthrax vaccination, E. This information shall read in the trifold brochure provided to potential vaccine recipients as follows: You may refuse anthrax vaccination under the EUA, and you will not be punished. No disciplinary action or adverse personnel action will be taken. You will not be processed for separation, and you will still be deployable. There will be no penalty or loss of entitlement for refusing anthrax vaccination. Nothing in law has changed to negate the authority of DoD members to refuse EUA COVID-19 drugs except the 6 civilian appointees engaged in willful misconduct against our Armed Forces. 11:51 PM · Sep 3, 2023  by Rose M. RohloffProviding informative snippets from 100,000s of primary source documents. None of this gain-of-function (GOF) work meets the legal definition of a vaccine. Link exhibit (A) with exhibit (C) regarding active substance; injections with GOF. Chimera used for creation, efficacy testing (human+animal); Humanized mice from injected aborted fetus cells, to create LUCIFERase encoded modRNA: active substance is SPIKE PROTEIN.
Exhibit (D): Pfizer document Rat testing - prior to human testing. Spike proteins in all organs with one (1) injection
World Council For Health - Detox Protocol https://worldcouncilforhealth.org/resources/spike-protein-detox-guide/
Flu shots 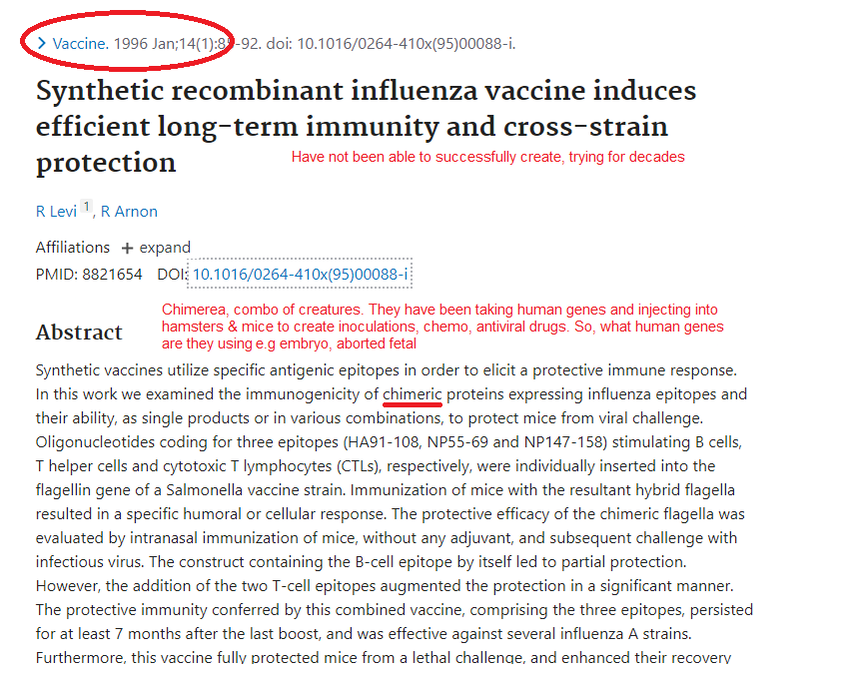
read blog entry 9/24/23 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||











by Rose RohloffWrite something about yourself. No need to be fancy, just an overview. The current fulminated issues of "hospital kidnapping", and denying Rights of parents has existed for decades. Now health systems are using Department of Children Family Services (DCFS) to enforce. The following are true, documented cases of families, spanning decades, fighting hospitals for the health of their children. |  |
In the Mid 1990s, a child was hospitalized in a Children's Hospital. "We had to fight the school system and the local Children's Hospital over coding of 'diagnosis' and school placement for our son: The only time we had to get a lawyer to fight against injustice. Our doctor said the underlying respiratory problem was allergy based, but the school system refused to place him in an environmentally safe school, with the local school having known poor air quality problems - a teacher was already being treated for recurring respiratory illness in the same classroom our child attended. We won. The doctor we trusted successfully identified our child's diagnosis and helped champion against the hospital. The hospital then sent us to a collection agency for refusal to pay for gross billing errors. When I called the collection agency and told them what we had already paid, they said we had overpaid. They told us to ask for an audit of the account and the result was that the hospital refunded us the money. When we requested in writing a copy of the whole medical record, the hospital sent without our name on it, and the postal service opened it. The hospital took a long time to respond to our complaint."
 Posted on X 7/25/24 by Kelly DNP Functional/Integrative Medicine | Bottom line: Don't mess with us especially regarding our kids WE KNOW HOW TO FIGHT!" quoted by parent-grandparent |
Another family with twins experienced an issue with the same hospital. "One twin was diagnosed with a malignant tumor at the base of her spine at about age three. The hospital did surgery. Everything looked good after that. Then, after recovering, the hospital insisted to do a series of chemo. After much prayer by the parents and our entire community, the parents discerned no, and had to fight the hospital. The parents won and the child grew up cancer free and graduated from high school without any further cancer."
In 2022, another case happened in a different state (as this is a national issue with health system conglomerations.) A young mother had a two year old child diagnosed with cancer. The latest lab came back White Blood Cell (WBC) of 2.8 (normal 4.5 to 11.0 × 109/L). The mother refused continued chemo treatment which would further drop her son's count. The child was not in protective isolation to add a layer of protection against being given an infection in the hospital. The hospital administrators called DCFS threatening her, along with her new six month old baby at home. This mother had to fight for proper care against open malpractice (if not manslaughter) of her child, with the hospital holding against the mother's will (medical kidnapping) with blatant coercion, threats and intimidation. With the correct second opinion and having to hire advocates, she was able to stop the care.
| Other parents, and children of elderly parents, across the country are experiencing similar situations of coercion, threats and intimidation from hospital administrators - including calling DCFS and the police; forcing families to hire expensive lawyers to even get a basic second opinion from a clinician they trust, and the stress with fear of actually having to go to court to fight for their loved one's Rights, who are being held (kidnapped) |  |
within the facility, violating the Right to leave against medical advice (AMA); and above all, hoping they do not die before a court ruling can be made.
Health systems have been providing admission forms upon entry in many cases, while people are under duress, to have them sign digitally without the time to review and understand "the fine print", when being handed an iPad or touch screen for the electronic record. Sadly, all persons, parents, family members need to stop and take the time to read the full admission forms, red line out and initial any portions they do not agree with, to exercise their legal Right of informed consent, Right to Try, for avoidance of any and all illegal coercion or undue influence by nurses, social workers, clinicians and administrators.
| One example of a form. A signed form should include the responsibility of hospital, staff enforcing quality care standards (e.g. to avoid hospital acquired infections and conditions), ensured care planning and care coordination, etc. Blanket consent is not informed consent, and should not include coercion upon ER visit with emotional compromised states. Being a signed form, a copy should always be immediately given to the person signing. | 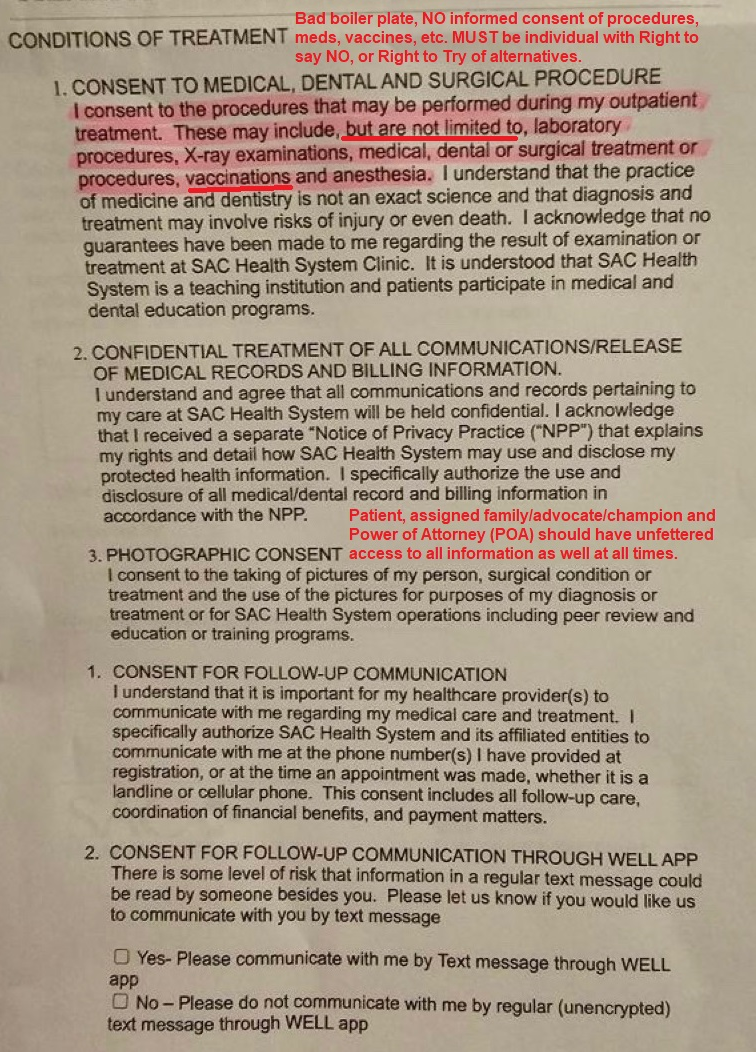 Example form from health system in California (boilerplate) |

by Rose Rohloff
| There are many classifications of drugs used for cardiac and vascular (CV) issues. A 2007 report is cited below, with his overviews by drug classification. The full article can be read with this link. |  |
"The use of cardiovascular medications can have a variety of neuropsychiatric consequences." Therefore, the following highlights are good review for anyone prescribed a CV drug, especially for the elderly, those with other conditions such as liver or kidney insufficiency, and/or also being prescribed psychiatric medications.
Neuropsychiatric Consequences of Cardiovascular Medications
by Dr. Jeff C. Huffman
Associate Professor of Psychiatry at Harvard Medical School and the Director of the Cardiac Psychiatry Research Program in the Massachusetts General Hospital (MGH) Division of Psychiatry and Medicine.
Angiotensin-converting enzyme inhibitors
"Bottom line: ACE inhibitors and angiotensin II receptor antagonists are associated with low rates of neuropsychiatrie side effects, though mood symptoms, psychosis, and delirium have been reported."
From snake venom to ACE inhibitor - the discovery of captopril- early 1980s, hypertension conferences were routinely enlivened by the poisonous Brazilian viper, Bothrops jararaca ... captopril — the first of the angiotensin-converting enzyme inhibitors, whose effects on blood pressure mechanisms mimicked those of the snake’s venom.
https://pharmaceutical-journal.com/article/news/from-snake-venom-to-ace-inhibitor-the-discovery-and-rise-of-captopril
https://pharmaceutical-journal.com/article/news/from-snake-venom-to-ace-inhibitor-the-discovery-and-rise-of-captopril
Beta-adrenergic blocking agents or Beta (β)-Blockers
"Bottom line: β-Blockers as a class are not clearly associated with depression; there is the most evidence for a propranolol-depression link, but even this relationship is equivocal. In contrast, β-blockers are associated with increased rates of fatigue."
Calcium channel blockers (CCBs)
"Bottom line: CCBs may be associated with fatigue in some patients, but otherwise cause few neuropsychiatrie symptoms."
Diuretics
"Bottom line: Diuretics most often cause neuropsychiatrie symptoms indirectly, through electrolyte abnormalities (thiazides) or vitamin deficiencies (loop diuretics). Acetazolamide is associated with fatigue and with delirium in renal failure."
Doctors should always monitor electrolyte levels (sodium/Na and potassium/K+) of their patients taking diuretics.
Doctors should always monitor electrolyte levels (sodium/Na and potassium/K+) of their patients taking diuretics.
Centrally acting agents - Antiadrenergic agent
"Bottom line: Clonidine is consistently associated with fatigue and sedation; delirium is infrequently associated with its use. (Clonidine) is also commonly used to reduce symptoms of opiate withdrawal.
Bottom line: Methyldopa is clearly associated with fatigue and sedation. In contrast to early studies linking methyldopa with depression, later reviews and studies have found this association to be relatively weak. Other neuropsychiatrie symptoms are uncommon.
Bottom line: Reserpine is associated with both sedation and daytime fatigue. Incidence of depression may be elevated among patients taking reserpine. However, other (generally more recent) reports question this association."
Bottom line: Methyldopa is clearly associated with fatigue and sedation. In contrast to early studies linking methyldopa with depression, later reviews and studies have found this association to be relatively weak. Other neuropsychiatrie symptoms are uncommon.
Bottom line: Reserpine is associated with both sedation and daytime fatigue. Incidence of depression may be elevated among patients taking reserpine. However, other (generally more recent) reports question this association."
α-Adrenergic agents
"Bottom line: Fatigue is the most common neuropsychiatrie side effect associated with -adrenergic antagonists; other neuropsychiatrie side effects are infrequent."
Vasodialtors
"Bottom line: Vasodilators are generally associated with low rates of neuropsychiatrie consequences. Hydralazine is a leading cause of drug-induced lupus, but this syndrome affects the central nervous system much less commonly than the idiopathic form of the disorder."
Antiarrhythmic medications
"Bottom line: Most Class I Antiarrthymic agents have been associated with psychosis and delirium in case reports. The syndrome of cinchonism associated with quinidine may include sensory changes along with delirium, and procainamide is a cause of drug-induced lupus.
Bottom line: Class III Amiodarone is associated with thyroid abnormalities in 15% of patients, and untreated thyroid dysregulation can lead to a variety of mood, cognitive, and psychotic symptoms. In contrast, direct neuropsychiatrie effects of amiodarone are uncommon.
Bottom line: Digoxin is associated with delirium and other cognitive effects, especially in toxicity. Visual changes and hallucinations may also occur with digoxin use, even at normal serum levels."
Bottom line: Class III Amiodarone is associated with thyroid abnormalities in 15% of patients, and untreated thyroid dysregulation can lead to a variety of mood, cognitive, and psychotic symptoms. In contrast, direct neuropsychiatrie effects of amiodarone are uncommon.
Bottom line: Digoxin is associated with delirium and other cognitive effects, especially in toxicity. Visual changes and hallucinations may also occur with digoxin use, even at normal serum levels."
Conclusion by Author
"... numerous cardiovascular medications can have neuropsychiatrie side effects, ranging from mood symptoms to cognitive effects to psychosis, and though a given agent may not consistently cause neuropsychiatrie symptoms in the general population, idiosyncratic reactions are possible." More specific studies are needed for, "clinicians ... to make fully-informed prescribing decisions for their patients."
Patients and their families know the cognitive baseline of individuals being prescribed medications, and therefore, should always monitor for any neuropsych impact seen if CV drugs are used, on an individual basis for what is safe per person. Any and all side effects should be know, along with contradictions to other drugs, for all medication being taken.
Patients and their families know the cognitive baseline of individuals being prescribed medications, and therefore, should always monitor for any neuropsych impact seen if CV drugs are used, on an individual basis for what is safe per person. Any and all side effects should be know, along with contradictions to other drugs, for all medication being taken.
* Dr Huffman is a professor of psychiatry at Harvard Medical School and the director of the Cardiac Psychiatry Research Program in the Massachusetts General Hospital (MGH) Division of Psychiatry and Medicine. He also serves as the associate chief for clinical services in the Department of Psychiatry at MGH.

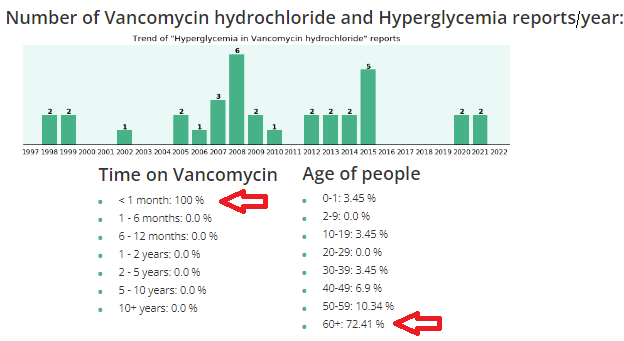
What should you be aware of regarding Vancomycin?
by Rose Rohloff
 | Vancomycin (Vanco) is an antibiotic, in the classification of Glycopeptide used for gram (+) bacteria, typically used for: Methicillin Resistant Staphylococcus Aureus (MRSA); Clostridium Difficile (commonly called C-diff), a potentially deadly infectious |
proliferation of the intestines (often after antibiotic use); and some hospitals are using as the standard protocol for elderly in the emergency room, for asymptomatic pneumonia, and other infections.
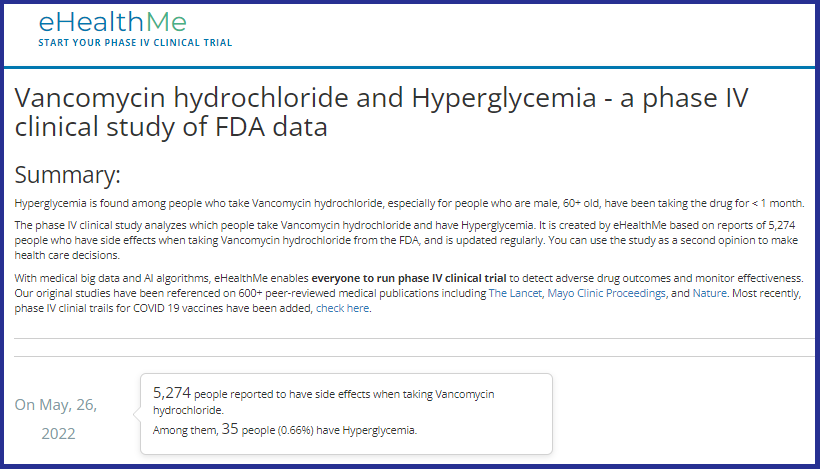
Clinicians (nurses, doctors, physician assistants, etc.) are supposed to do comprehensive history and physicals (H&Ps) before using any drugs or treatments. And, it is important to know underlying conditions before using Vanco, because it can raise glucose levels, especially in diabetics, and/or cause kidney (renal) insufficiency, especially in elderly.
Clinicians (nurses, doctors, physician assistants, etc.) are supposed to do comprehensive history and physicals (H&Ps) before using any drugs or treatments. And, it is important to know underlying conditions before using Vanco, because it can raise glucose levels, especially in diabetics, and/or cause kidney (renal) insufficiency, especially in elderly.
The following use case is regarding an admitted primary care doctor as the patient.
"I don't know what the average "lay person" does when they don't have all this information, and without a medical person to look out for them."
"This article is exactly why they stopped Vanco when he had his MRSA infection. His kidneys were starting to get compromised, so they immediately stopped it and started him on a different antibiotic, Daptomycin, which worked just as well and had less side effects for his kidneys and diabetes. Thankfully they caught it very early because of the blood tests they were doing to see what was happening. The new antibiotic was infused only once a day as opposed to twice a day Vanco, and there weren't all the extra blood draws to make sure the kidneys and glucose were doing okay. God is really in control and watching out for us, because the medical field doesn't always do that, even with a fellow medical person."
"I don't know what the average "lay person" does when they don't have all this information, and without a medical person to look out for them."
"This article is exactly why they stopped Vanco when he had his MRSA infection. His kidneys were starting to get compromised, so they immediately stopped it and started him on a different antibiotic, Daptomycin, which worked just as well and had less side effects for his kidneys and diabetes. Thankfully they caught it very early because of the blood tests they were doing to see what was happening. The new antibiotic was infused only once a day as opposed to twice a day Vanco, and there weren't all the extra blood draws to make sure the kidneys and glucose were doing okay. God is really in control and watching out for us, because the medical field doesn't always do that, even with a fellow medical person."
Vanco and high glucose/hyperglycemia
 |  |
Vanco and kidney (renal) failure
Changes in vancomycin use in renal failure Stefaan J Vandecasteele 1, An S De Vriese pub in 2010
Abstract A progressive increase in vancomycin resistance with consequent treatment failure has been observed in staphylococci. Therefore, new dosing guidelines advocating much higher vancomycin doses have been issued. Target trough levels of 15-20 microg/ml are proposed. Whether and how these targets can be achieved in patients with chronic kidney disease or those on dialysis are still under evaluation. The higher vancomycin doses to achieve these treatment targets carry a substantial risk for nephrotoxicity. This risk is incremental with higher trough levels and longer duration of vancomycin use. Critically ill patients, patients receiving concomitant nephrotoxic agents, and patients with already compromised renal function are particularly at risk for vancomycin-induced nephrotoxicity.
Abstract A progressive increase in vancomycin resistance with consequent treatment failure has been observed in staphylococci. Therefore, new dosing guidelines advocating much higher vancomycin doses have been issued. Target trough levels of 15-20 microg/ml are proposed. Whether and how these targets can be achieved in patients with chronic kidney disease or those on dialysis are still under evaluation. The higher vancomycin doses to achieve these treatment targets carry a substantial risk for nephrotoxicity. This risk is incremental with higher trough levels and longer duration of vancomycin use. Critically ill patients, patients receiving concomitant nephrotoxic agents, and patients with already compromised renal function are particularly at risk for vancomycin-induced nephrotoxicity.
Acute kidney injury during daptomycin versus vancomycin treatment in cardiovascular critically ill
Conclusions: Daptomycin appears to be safer than vancomycin in terms of AKI risk in ICU patients treated for cardiovascular procedure-related infection. Daptomycin could be considered as a first line treatment to prevent AKI in high-risk patients. NIH 2019

by Rose Rohloff
An India folklore, regarding lack of awareness, demonstrates the current myopic view of various specialists, who look at isolated symptoms without comprehensive assessments, resulting in poor or lack of diagnosing of real issues to address in patients. The industry push to eliminate primary care, teaching people they don’t need a primary doctor, or using primary care doctors as simple pass-through without diagnosing, handing off to multiple other doctors, has resulted in the loss of care coordination, overdosing multiple medications with contraindications/side effects, with increased conditions because multiple doctors only look at their individual view.
An India folklore, regarding lack of awareness, demonstrates the current myopic view of various specialists, who look at isolated symptoms without comprehensive assessments, resulting in poor or lack of diagnosing of real issues to address in patients. The industry push to eliminate primary care, teaching people they don’t need a primary doctor, or using primary care doctors as simple pass-through without diagnosing, handing off to multiple other doctors, has resulted in the loss of care coordination, overdosing multiple medications with contraindications/side effects, with increased conditions because multiple doctors only look at their individual view.
The following version of the blind men and the elephant story is from Peacecorp.gov, and is analogous to the existing healthcare system of specialists.
Long ago, old blind men were curious about the many stories they heard about elephants. The men were led to one for each person to independently touch the animal.
Long ago, old blind men were curious about the many stories they heard about elephants. The men were led to one for each person to independently touch the animal.
- The first blind man reached out and touched its side. "An elephant is smooth and solid like a wall!" he declared. "It must be very powerful."
- The second blind man put his hand on the elephant's limber trunk. "An elephant is like a giant snake," he announced.
- The third blind man felt the elephant's pointed tusk. "I was right," he decided. "This creature is as sharp and deadly as a spear."
- The fourth blind man touched the elephant's leg. "What we have here," he said, "is an extremely large cow."
- The fifth blind man felt one of its giant ears. "I believe an elephant is like a huge fan or maybe a magic carpet that can fly over mountains and treetops," he said.
- The sixth blind man gave a tug on the elephant's coarse tail. "Why, this is nothing more than a piece of old rope." he scoffed.
| The six blind men determined what they knew on limited assessment of only touching one part of the elephant, just as individual doctors only look at single symptoms; for example, cardiologist only looks at the heart, nephrologist only looks at kidney, endocrinologist only looks at the endocrine system ... |  |
All body systems impact each other, designed to function as a whole, for a well orchestrated, compensatory mechanism. By only looking at individual symptoms of isolated systems, patient’s underlying conditions are not addressed for health, and can often be fulminated and/or obscured by medications. And, the reason primary care doctors are imperative for knowing the whole patient, knowing how to diagnose and treat many conditions. Primary doctors should only pass their patients to specialists for complicated, complex conditions, while always following their patient and maintaining all coordination with any other doctors.

by Rose Rohloff
Calm intelligence, professionalism, logic and sense. Nine (9) doctors interviewed https://www.bitchute.com/video/2JPy7qZiXvNr/ regarding Covid, Hydroxychloroquine (HCQ) and masks.
Calm intelligence, professionalism, logic and sense. Nine (9) doctors interviewed https://www.bitchute.com/video/2JPy7qZiXvNr/ regarding Covid, Hydroxychloroquine (HCQ) and masks.

| by Rose Rohloff We need to change the dialogue, remove panic. This is a virus that can infrequently lead to death, as opposed to "a deadly virus." If this veteran can fight it off, so can millions of people focused on strengthening their immune systems. |  |
With perpetual reporting of the COVID-19 virus, there has been a lot of panic reaction from the public, fostered by the media, as well as from local clinical staff. These reactions have brought existing issues in the healthcare system to the forefront, that we can address go forward, especially for discernment to champion better quality of care. The following two use case examples happened last week, which demonstrate panic reactions from clinicians, the need for good primary care, and the need to address care standards, especially in crisis, with sense at the delivery level.
An immune suppressed mother has three children, one being a 10 yr. old daughter who woke with a 102 temperature and a sore throat. The mother is not reactionary, having good instinct regarding when her children are fighting off bugs, building up their immune systems. She phoned the pediatrician to ask for testing if it is strep or a virus. The pediatrician stated they only test for COVID-19 if someone is hospitalized, and they would not do a strep test, “Don’t bring your child in”, and then the pediatrician went on a rant about social distancing, “This virus will not end …” (with no reported cases in the area) etc. and simply ordered Amoxicillin.
 | The mother phoned me commenting, "I don't feel comfortable with this situation, the doctor's reaction and their approach. |
I don't want to give my daughter an antibiotic if she doesn't need it, and especially if it is a virus, let alone the Corona virus." Removing all emotion from the situation with her, we discussed getting zinc in EZC Pak from the CVS a mile away, that she could pick up via their drive through, along with foods high in Vitamin A to boost her daughter's immune system. I also called the local Urgent Care center explaining the situation: a mother immunosuppressed, her daughter is in the EMR system, she just wants a strep swab to avoid unnecessary antibiotics, to please have a nurse do the swab through the car window when she drives up - avoiding any cross contamination issues. They stated no problem.
| The mother called the Urgent Care center and they informed her she got bad information, they would absolutely not do a swab from the car, she must come in. She stated, “You want me to walk into that center with sick people along with my two other smaller, healthy children so in less than a minute you can swab my other daughter’s throat to verify if she needs an antibiotic?” They told the mother that she could not bring that many people into the facility with her. The mother asked, “What exactly to do you expect me to do then to protect myself, and what do you want me to do with my other kids?” The healthcare personnel demonstrated panic, without some basic sense. I finally asked the mother what she wanted to do. She stated, “My daughter is alert, drinking, not that bad. I am going to get Zinc and good foods, push fluids especially with warm lemon and honey, have her gargle with warm salt water, and see how she is in 24 hours.” The daughter’s temperature was 99 by nightfall, and 98 degrees by the next day without a sore throat. If the mother had not questioned the panic of the doctor and nurse, her daughter would have been put on an unnecessary antibiotic, opening her up to secondary infections, and exposing herself to unnecessary virus and bacteria while being immunosuppressed. | From the NIH Amoxicillian: Additionally, there is a moderately increased risk of secondary Clostridium difficile (C-diff) colitis when compared with other classes of antibiotics. Females taking this medication can also develop vaginitis secondary to vaginal mycosis or candidiasis. (Our bodies keep C-diff and candidiasis in check with our needed good bacteria.) The next day, the mother stated, "The doctor lost all credibility with me going on in a panic about the issues with the COVID-19, "this will never end by Easter, etc." when the hospitals have little volume, no reported cases. "She refused to do any history and basic assessment to swab my daughter to rule out strep before writing a prescription." Our healthcare system has been broken regarding the lack of some basic sense at the ground level, with reactionary versus proactive care; missing great primary care doctors, avoiding the quick symptom = writing a prescription form of care.  |
The same week, a second mother of four small children, one being a seven year old who was having sore joints and some blood in her urine. The doctors in Green Bay did a wonderful job of a full, very detailed history and then exam with targeted tests, quickly diagnosing Rheumatic Fever. Her and her other three, healthy children were instructed to do proactive strep testing since they all had close exposure with the daughter. "The center made us feel like lepers. Instead of simply coming out to the car to meet us, they brought us to an empty lobby with a nurse who came out in a full hazmat suit to do simple strep swabs. The nurse freaked out when my son simply cleared is throat, creating anxiety, complaining, "He just coughed."
The clinicians throughout both cases should have been calming, simply asking good questions, and then only ordering the correct test before ordering medication. And, in both cases, clinicians could have had the tests quickly, avoiding the waste of hazmat gear, not frightening healthy family members as well as not exposing them to potential germs in the health facilities - avoiding cross contamination issues.
What we need to focus heavily on:
- Great education nationally in diet to strengthen the immune system. Great nutrition understanding regarding what vitamins to focus on, removal of sugars from the diet, etc. The idea of waiting on vaccines after the fact, for every virus, is not realistic or proactive.
- Better testing of high risk patients regarding their health with focus on strengthening their own immune system.
- Zinc and other nutrients when one is immediately feeling poor. Fights inflammation, works with immune system or exposure to infectious persons.
 Replay video, with permission via Dave Chase, Health Rosetta https://vimeo.com/403748057/1b07436d73 | Health Rosetta hosted a wonderful webinar with Chief Medical Officers (CMOs) from around the country speaking, without panic, about the effective care of their patients at home with COVID-19. Their stories demonstrating the importance of shifting back to great primary care. |
One point stood out regarding their focus that is so often missing in health systems: seeing 'clean' patients first, and then seeing contagious patients grouped together, ensuring avoidance of cross contamination, and minimizing the volume of masks, gowns or hazmat suits used.
Hopefully, many good things will come from this virus experience to positively shake up our healthcare system, including basic sense procedures, with the importance to rebuild and focus on great primary care again. Another glaring issue to address is the role of clinicians as cool, calm professionals, removing emotion when instructing with full information, with clearly explained options for informed consent and decision-making for delivery of quality care.
Hopefully, many good things will come from this virus experience to positively shake up our healthcare system, including basic sense procedures, with the importance to rebuild and focus on great primary care again. Another glaring issue to address is the role of clinicians as cool, calm professionals, removing emotion when instructing with full information, with clearly explained options for informed consent and decision-making for delivery of quality care.

by Rose Rohloff
Championing care: knowing your individual baselines, understanding trending deviations, influencing factors.

| A Wall Street Journal (WSJ) article https://lnkd.in/e9awgQT 1/24/2020 posted wrote: "Nearly 150 years ago, a German physician analyzed a million temperatures from 25,000 patients and concluded that normal human body temperature is 98.6 degrees Fahrenheit. That standard has been published in numerous medical texts and helped generations of parents judge the gravity of a child’s illness. But at least two dozen modern studies have concluded the number is too high. Or was it? In a new study, researchers from Stanford University argue that Wunderlich’s number was correct at the time but is no longer accurate because the human body has changed. Today, they say, the average normal human-body temperature is closer to 97.5 degrees Fahrenheit." | Championing your own health is about understanding your healthy baselines. Just as individuals have a variable "healthy" baseline for their blood pressure and heart rate, why would an individual not have an individualized, normal baseline for their temperature? And, temperatures are now measured using different methods: forehead-ear-mouth-rectal, producing deviations based upon how the temperature is obtained. It is important to understand, compare what mechanism was used to take the temperature. Is your normal 98 degrees, while another may run 97 degrees? Is the person normally running 97 degrees now have a temp of 99 along with malaise, dehydration because they are fighting a virus or bacteria? Assessment/vital sign numbers provide more information for clinicians (Doctor, PA, Nurse, etc.) when provided in context of associations, trends, baselines and influencing factors. |

by Rose Rohloff
It is known taking medications will impact various lab values. For example, Diuretics e.g. Lasix (Furosemide), can cause low potassium levels. There is an interesting article in Medscape, Which Drugs Interact With Lab Tests? Jun 18, 2019., addressing the fact that certain medications can also interact with the actual processing of certain lab tests causing inaccurate results.
It is known taking medications will impact various lab values. For example, Diuretics e.g. Lasix (Furosemide), can cause low potassium levels. There is an interesting article in Medscape, Which Drugs Interact With Lab Tests? Jun 18, 2019., addressing the fact that certain medications can also interact with the actual processing of certain lab tests causing inaccurate results.
A recent view of the prescribing information for 1368 prescription drugs found that 134 (9.8%) included information about a specific lab test interaction, 31 (2.3%) stated that the drug did not interfere with lab tests, and four stated that there was no available information.[1] ... |  Patients, families and caregivers need to be aware of what name, class, internal action, as well as all other medication interactions for every medication, vitamin and supplements being taken. As Dr. Scott shares as insightful, it is also important before getting lab values done to understand if any medications being taken will impact labs to be processed and cause false results. |

by Rose Rohloff
The 2009 HITECH Act and the Center for Medicare Medicaid Services’ (CMS) Meaningful Use regulations caused a massive spend for electronic medical records (EMRs), the push for interoperability, as the solution to healthcare quality. However, EMRs are not solutions - along with massive IT overhead spend with decreasing quality - because in a high percent of instances, nurses and doctors don’t even read them.
A 40-year old mother went to the doctor after treating herself holistically for some laryngitis, stuffy nose, congested sinus, with continued symptoms after five days. After an exam, the doctor stated, “I am not going to give you antibiotics. You do not have a fever; your lungs sound clear. It looks like a little virus with severe allergies. I recommend an antihistamine.” The patient told him, “Thank you for not putting me on antibiotics when they are not needed, that makes me happy.” He responded, “I am glad you are glad.”
A 40-year old mother went to the doctor after treating herself holistically for some laryngitis, stuffy nose, congested sinus, with continued symptoms after five days. After an exam, the doctor stated, “I am not going to give you antibiotics. You do not have a fever; your lungs sound clear. It looks like a little virus with severe allergies. I recommend an antihistamine.” The patient told him, “Thank you for not putting me on antibiotics when they are not needed, that makes me happy.” He responded, “I am glad you are glad.”
He then said something and the patient responded, “I have MS.” He responded, “Oh wait, you have Multiple Sclerosis?”
This story is sadly too often the new normal, numerous instances of patients and their caregivers stating issues of diagnosing with medication prescription, or misdiagnosis; the doctor or nurse having no idea of pre-existing conditions or a full list of medications currently being taken, a lack of care coordination or care planning because the time was not taken to simply read the chart (whether written or electronic), and ensuring a comprehensive history followed by the necessary physical assessment.
No physician or nurse should walk in to care for a patient without first having read the patient’s record, knowing all current information, the last visit/healthcare encounter, chronic conditions/comorbidities, and all medications; then, asking for updates of changes. Unfortunately, even without having to decipher poor handwriting, being able to read clean typed text, clinicians are not simply reading the basics of information they should before doing any diagnosis, planning and care, or prescribing of medications.
This story is sadly too often the new normal, numerous instances of patients and their caregivers stating issues of diagnosing with medication prescription, or misdiagnosis; the doctor or nurse having no idea of pre-existing conditions or a full list of medications currently being taken, a lack of care coordination or care planning because the time was not taken to simply read the chart (whether written or electronic), and ensuring a comprehensive history followed by the necessary physical assessment.
No physician or nurse should walk in to care for a patient without first having read the patient’s record, knowing all current information, the last visit/healthcare encounter, chronic conditions/comorbidities, and all medications; then, asking for updates of changes. Unfortunately, even without having to decipher poor handwriting, being able to read clean typed text, clinicians are not simply reading the basics of information they should before doing any diagnosis, planning and care, or prescribing of medications.

by Rose Rohloff
| This needs to be addressed at the State & Federal levels - fighting the unconstitutional Federal violation of the Sherman Antitrust Act of 1890 by Congress and the Executive Branch. [The Federal Gov is also violating pushing for Narcan to be in every household - pouring gasoline on fires - because now people think they can be saved continuing to overdose on street drugs, especially Fentanyl: read NARC PARTY - OPIOID CRISIS AND SURGEON GENERAL ADVISORY | How Mylan, the maker of EpiPen, became a virtual monopoly - The Washington Post washingtonpost.com› business › economy › 2016 › 08 › 25 › 7f83728a-6aee-11e6-ba32-5a4bf5aad4fa_story.html August 26, 2016 - The company lobbied lawmakers — both directly and indirectly — to increase the availability of epinephrine autoinjectors in U.S. schools. |
Use Case: A police officer was having hives and went to an emergency room. The staff asked him if he wanted an EpiPen. His response, "What the hell is it? The staff did not educated him, provide one to him to use if he felt he needed it. I informed him to read the fine print = it was a dose for a child an not a grown 200lb man, with an expiring date in a couple of weeks.
| On November 13, 2013, President Obama signed into law the School Access to Emergency Epinephrine Act. The federal legislation provides a financial incentive for states to enact their own laws requiring schools to keep non-student specific epinephrine auto-injectors in case of an emergency. And so, the Federal Government created an illegal monopoly for company who owns the patented auto-injector, not the medication, followed by price gouging, especially for times of crisis, and finally panicked outrage in the public. |  2024 pricing https://entirelypetspharmacy.com/epinephrine-injection-1-to-1000-sterile-multi-dose-vial-50ml.html
|
| 'There's nothing to give them': Patients, pharmacists scrounging for EpiPens Full story Patients and pharmacists nationwide are grappling with a persistent shortage of Mylan's EpiPen, forcing some to travel great distances or go through several hoops to access the lifesaving allergy treatment, according to Bloomberg. EpiPens have been difficult to obtain since at least May 2018, when the FDA alerted the public to the shortage. | 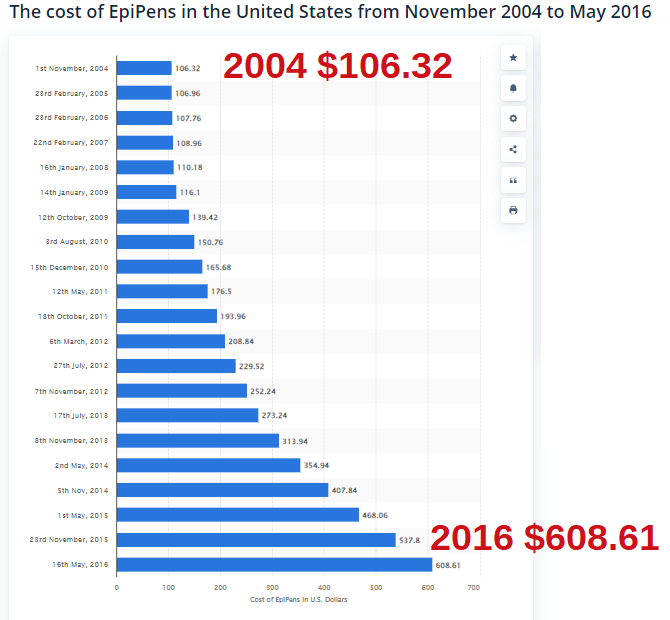 Updated price Jan 2024 https://www.drugs.com/price-guide/epinephrine# |
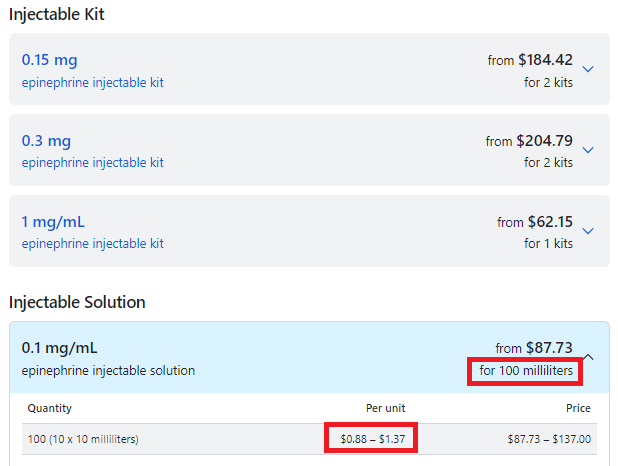
 Generic = vial, https://www.emsstuff.com/epinephrine-1mg-vial-anaphylaxis/ 2024 price | Cheaper "do-it-yourself" alternative EpiPen may carry more ...https://www.cbsnews.com/news/cheaper-epipen-alternative-may-carry-risks/ The cost is about $20 - $15 for a syringe and $5 for a vial or two of the drug. |
Summary
- Obama signed into law an illegal monopoly
- The Mylan company does not control the patent on the drug epinephrine, only their autoinjector Epipen.
- Epinephrine comes in multi-does vials: EpiPens are only single dose!
- CDC stats read 4%-6% have food allergies, only .001 of the population has anaphylaxis to nuts + shell fish, the biggest allergy issues, 63 to 99 deaths occur each year in the United States due to anaphylaxis.
by Rose Rohloff
The baby boomer generation is now the growing population of elderly with more care needs in home health. As the current generation is being faced with the care responsibilities, many are still unaware concerning various facets of caring for others: advanced directives and living wills; stimulation and diets for mental sharpness, questions to ask and quality of care considerations with becoming power of attorneys - the core of healthcare awareness. One area is focused heavily within hospitals and other care delivery environments, but yet over looked in private homes – surface areas and cleanliness.
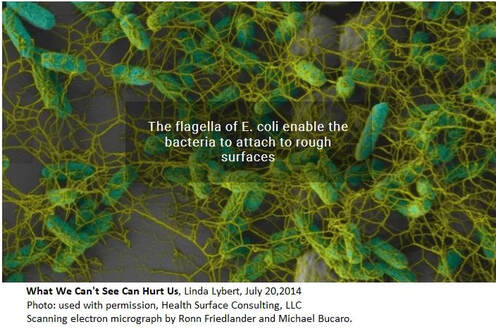
A popular trend in houses is the use of marble and granite as counter tops. A leading surface expert, Linda Lybert President of Healthcare Surface Consulting stated, “Granite and Marble are like large sponges you cannot wring out.” The photo displayed shows the build up of E. coli bacteria in the pores of stone. According to Ms. Lybert, even when sealed, the porousness is reduced, but not eliminated. And, bleach is not able to eliminate once they reside in the crevices.
A popular trend in houses is the use of marble and granite as counter tops. A leading surface expert, Linda Lybert President of Healthcare Surface Consulting stated, “Granite and Marble are like large sponges you cannot wring out.” The photo displayed shows the build up of E. coli bacteria in the pores of stone. According to Ms. Lybert, even when sealed, the porousness is reduced, but not eliminated. And, bleach is not able to eliminate once they reside in the crevices.
All surfaces in the home, counter tops, floors including laminates, tile and grout need diligent daily cleaning and disinfection. However, Ms. Lybert brings awareness that regarding "stone surfaces, including granite/marble, there is no effective means to disinfect these surfaces." Consider, "granite is an underground aquifer for our water filtering out all kinds of things. Given the right kind of environment, heat and moisture, bacteria will grow."
As the elderly begin to lose their mobility and agility, it is important to maintain clean surfaces in bathrooms and bedrooms, along with the most important surface being the skin. Diligent hand washing and bathing is important throughout the day to avoid cross contamination from the loved one you are caring for, as well as to them. The other surface area to be conscientious of is bedding. When excrement accidents occur, it is important to wash bedding with very hot water to not only clean them, but also kill the microbes.
Clostridium difficile (commonly known as C-diff) "is in the community and found in outpatient settings. There are significant risk factors in patients who are immunosuppressant, individuals who have been on antibiotic therapy, and the elderly population." C-diff is a secondary, very dangerous and potentially deadly infection after antibiotic use. [read article] It is important to those in the community to have appropriate antibiotic prescriptions and use, especially avoiding unnecessary broad spectrum antibiotic use which targets the "good" bacteria you need internally (and not on external surfaces) to kill off C-diff.
As the elderly begin to lose their mobility and agility, it is important to maintain clean surfaces in bathrooms and bedrooms, along with the most important surface being the skin. Diligent hand washing and bathing is important throughout the day to avoid cross contamination from the loved one you are caring for, as well as to them. The other surface area to be conscientious of is bedding. When excrement accidents occur, it is important to wash bedding with very hot water to not only clean them, but also kill the microbes.
Clostridium difficile (commonly known as C-diff) "is in the community and found in outpatient settings. There are significant risk factors in patients who are immunosuppressant, individuals who have been on antibiotic therapy, and the elderly population." C-diff is a secondary, very dangerous and potentially deadly infection after antibiotic use. [read article] It is important to those in the community to have appropriate antibiotic prescriptions and use, especially avoiding unnecessary broad spectrum antibiotic use which targets the "good" bacteria you need internally (and not on external surfaces) to kill off C-diff.

by Rose Rohloff
But, what is value? Is society conditioned to accept low quality as value, because a lower standard has become the norm?
| Value is a relative term based upon personal perception, and oftentimes great marketing. True value is based upon insightful knowledge of what entails quality along with the cost of delivering goods and services. Value-based care is the new buzz for basing reimbursement in the healthcare industry. But again, what is value care: personal perception, marketing, cost? |  |
This article was conceived after several conversations regarding what defines quality care, with veteran clinicians (nurses and doctors), insurance brokers, as well as numerous 40-80 year olds who make up the typical population across the country. Using the following encounter as an example, I want to review what determines true value of care delivery compared to the normal perception being marketed.
A surgeon office within a surgical center, (the surgeon with privileges at two leading health systems), has 5-star Healthgrades ratings, including comments: the staff is courteous; appointments start on time; the Physician Assistant (PA) is very intelligent, knowledgeable, articulate and caring; and the surgeon with a benchmark performance staff. There are also one star ratings including a comment the staff is not properly trained and do not know how to maintain a sterile environment.
The primary issue with such score deviations is determining if poor marks are isolated instances (one offs); or, if the variance of only highest and lowest reflect the knowledge of reviewers. Are the high ratings from non-healthcare persons based on perception of the veneer friendliness and scheduling, with one star comments based on specific quality requirements, care competency posted by those with healthcare insight/experience?
As a 35+ year healthcare veteran, an answer was determined accompanying a Medicare patient ‘John’, in his mid-80s who experiences early stage dementia, to the office for a post-op visit for a leg stint placement.
The primary issue with such score deviations is determining if poor marks are isolated instances (one offs); or, if the variance of only highest and lowest reflect the knowledge of reviewers. Are the high ratings from non-healthcare persons based on perception of the veneer friendliness and scheduling, with one star comments based on specific quality requirements, care competency posted by those with healthcare insight/experience?
As a 35+ year healthcare veteran, an answer was determined accompanying a Medicare patient ‘John’, in his mid-80s who experiences early stage dementia, to the office for a post-op visit for a leg stint placement.
| Upon arriving, another elderly patient (80s) was sitting outside, unattended in wheelchair, hot sun, 100 degree weather, no water. When asked why he was there, he stated, “I can’t stand the freezing air conditioning inside while waiting for a ride.” After walking John into the lobby, the gentlemen clearly seen through the glass door was pointed out to the receptionist stating that he was left in hot sun, no water, unattended. The receptionist stated, “It is his choice to stay out there.” I then stated, “Get someone to check on him, give him water, put him in the shade and check when his ride is supposed to arrive and monitor him if it is delayed or bring him inside.” One person escorted us back to exam room. She did not introduce herself or her title. She proceeded to take the blood pressure with no other vital signs (unknown if a secretary, an aide, a nurse or tech). She then asked the patient, “How much do you weigh?” He gave a number. As patient champion I responded, “He doesn’t know, he has not weighed himself. You need to weigh him yourself.” She responded, “We don’t have a scale.” She then left. I followed her witnessing her documenting the incorrect data. | I reiterated he has dementia with no idea how much he weighs. She replied, “It doesn’t matter anyways, we just need to put something in the record.” She was reflecting an 11 pound weight loss from previous recording. It is unclear if they performed the previous weighing, if it was done just prior to surgery to determine proper anesthesia delivery for his surgery.  Another woman in scrubs entered the exam room without introducing herself or her title, asking John to remove his shoes and socks. (The scheduled appointment was with the PA so the patient assumed her identity.) She asked him if his wound was healed and he replied, “Yes.” She documented something in the chart without ever assessing his wound for healing or determining if there was infection. She bent down and felt his feet with her whole hands stating they feel warm, and then asked if he had numbness in his feet. John responded, “Yes.” | Having worked as a registered nurse (RN) in cardiovascular and neuro intensive care units (ICUs), I know she never did pedal (foot) pulse checks x4 comparing both feet. She never assessed location of numbness, or if chronic/intermittent, positional with sitting/, standing, walking, etc. The family had asked if aspirin could be stopped as the patient has experienced nose bleeds in the past. The staff person responded yes and since there was 90% blockage of the previous stint, it was cleaned out and continue Plavix. There was no establishment of lab work as part of care plan determining effectiveness of the medications, especially since the previous stint occluded. "1,750 or so stent patients are also prescribed Plavix to prevent clots from forming around the stent, but of that group, approximately 500 (29%) carry a genetic variation that prevents them from converting Plavix into its active form. This gene-related lack of response stands to be "especially severe" in about 50 (3%) of those patients, who won't derive any benefit from Plavix - 2010 Vanderbilt Medical Center |
She then stated they would be ordering an ultrasound as a standard post-op test to determine the effectiveness of the stint - over three weeks after the procedure.
Why didn't they do the ultrasound during the post-op visit to have results to make sure the stint was effective? No doppler was used to assess extremity blood flow.
She stood up, touched the paperwork, the marker and laminate sheet then touched the door handle leaving – never having washed her hands before assessing the patient, nor after putting her hands on his feet.
Perceived value based on quality versus true value and cost
The office visit was charged to Medicare, with an elderly patient perceiving the staff as nice during the office visit.
The care competency and quality as true value-based care during the visit includes:
- lack of basic cleanliness standards with severe cross contamination practices
- no introduction of name or title of any staff member
- fraudulent documentation in the electronic medical record (EMR)
- no assessment performed during a specific post operative visit (a family member could have taken the BP and said his feet felt warm.)
- lack of care planning and evaluation of medication regime
- unnecessary secondary office visit charging for follow up
- another elderly patient left unattended in the hot sun
If the U.S. healthcare system wants to achieve true value-based care, we need an educated population, higher accountability of staff standards with the ability to send evaluations direct to payers based on specific facts and not emotion, and surveys must include care competency reviews versus only veneer questions of politeness, room appearances, and on time scheduling.
The care competency and quality as true value-based care during the visit includes:
- lack of basic cleanliness standards with severe cross contamination practices
- no introduction of name or title of any staff member
- fraudulent documentation in the electronic medical record (EMR)
- no assessment performed during a specific post operative visit (a family member could have taken the BP and said his feet felt warm.)
- lack of care planning and evaluation of medication regime
- unnecessary secondary office visit charging for follow up
- another elderly patient left unattended in the hot sun
If the U.S. healthcare system wants to achieve true value-based care, we need an educated population, higher accountability of staff standards with the ability to send evaluations direct to payers based on specific facts and not emotion, and surveys must include care competency reviews versus only veneer questions of politeness, room appearances, and on time scheduling.

PART 1 of 4: THE A, B, C of U.S. GOVERNANCE
by Rose M. Rohloff
Across the country I have asked various parents, teachers, grade school and high school students an elementary question: "What form of government is the United States?"
Being the most basic of query, the universal response of “A Democracy” took me by surprise. The next request was for each person to quote the Pledge of Allegiance. Some did not know it clearly, while others did recite ... United States of America, and to the Republic for which it stands ... followed by, "Oh, so what."; "It is a democratic republic which is the same as a democracy." One male in his twenties from Chicago (who stated he attended the best high school in the city) responded, "Well, we need a combination democracy, socialist, communist government because people are too stupid to think for themselves." My final statement to this person was to point out that these are three opposing ideologies that cannot exist together.
The question begs to be asked, "How can voters function as responsible citizens and make reasoned, insightful judgment when voting, if they do not know or understand what form of government exists in the United States?"
It is interesting to compare the intelligence of writing for grade school children from the 1800s with the readings of today. Children in the 1800s were educated in civics starting at young ages, because parents and grandparents fought to obtain and secure for them the new form of government - a Republic governed by a national Constitution.
Being the most basic of query, the universal response of “A Democracy” took me by surprise. The next request was for each person to quote the Pledge of Allegiance. Some did not know it clearly, while others did recite ... United States of America, and to the Republic for which it stands ... followed by, "Oh, so what."; "It is a democratic republic which is the same as a democracy." One male in his twenties from Chicago (who stated he attended the best high school in the city) responded, "Well, we need a combination democracy, socialist, communist government because people are too stupid to think for themselves." My final statement to this person was to point out that these are three opposing ideologies that cannot exist together.
The question begs to be asked, "How can voters function as responsible citizens and make reasoned, insightful judgment when voting, if they do not know or understand what form of government exists in the United States?"
It is interesting to compare the intelligence of writing for grade school children from the 1800s with the readings of today. Children in the 1800s were educated in civics starting at young ages, because parents and grandparents fought to obtain and secure for them the new form of government - a Republic governed by a national Constitution.
| Arthur J. Stansbury created the Catechism on the Constitution (the “Catechism”, Boston 1828) that was used to teach schoolchildren. | Today, Magruder's American Government is “hailed as a stellar educational resource for nearly a century, updated annually to meet the changing needs of today's high school students and teachers. The program's engaging narrative is enhanced with numerous primary sources, political cartoons, charts, graphs, and photos …” [Amazon] |
The Catechism, written for grade school aged children, does not contain pictures or cartoons, and has elegant writing in the form of Question followed by Answer. A few of the profound sentences by Stansbury summarizing poignant points for me include:
- "That a people living under a free government which they have themselves originated should be well acquainted with the instrument which contains it ... this would be no good reason why pains should not be taken to understand and to imprint (the Constitution) upon the mind ... its brevity surpassing all example, it is certainly a most reprehensible negligence to remain in ignorance of it." (Preface)
- "Let every American learn, from his earliest years, to love, cherish and obey the Constitution. Without this he can neither be a great or a good citizen." (Page 10)
- Question: "But if even the Congress itself should make a law which is contrary to the Constitution, must the people obey it? Answer: No." (Page 11)
In contrast, today’s American Government book by Magruder's teaches:
Figure 1: www.slader.com/textbook/9780133240825-magruders-american-government/18/
- U.S. Government is taught as being a Representative Democracy versus specifically a Republic (which is not discussed), and describes the various forms in rudimentary text, without addressing the ideologies in depth.
- Communism is not discussed especially in relation to China, the Chinese Communist Party (CCP). The various forms of Government in detailed ideology should be Democracy, Republic, Socialism, Communism, Dictatorship, Monarchy, Tribal.
- Specific ideologies variations are not defined well and the writers are focused on side-by-side listing of dictatorships to democracy, with lack of detailed distinctions.
The comparison of "new" (incorrect) teaching is important, because Democracy intentionally does not appear anywhere in the Declaration of Independence or the Constitution. [Cato Institute: On Democracy Versus Liberty, By Steve H. Hanke, Feb 2011] The founders studied history in depth with types of governments, and specifically did not create a democracy to avoid mob rule.
The public today is often bombarded with reports, news (non-news) - an overabundance of opinions regarding important issues. Without the basic understanding of the U.S. Republic, individuals have been conditioned to react with and vote based on emotion, as opposed to thoughtful reasoning; the breaking down of issues with intelligent discourse based on Constitutional understanding.
Authors have broken down a differentiation of a democracy in the simplest term as a majority dictating issues. When a majority of persons are swayed with emotion, it is ‘mob rule’. This distinction is important, as more and more voters are craving socialism, with groups such as ANTIFA and #xyzMOVEMENTS continuing to form. The Founding Fathers researched all the various forms of governments thoroughly before specifically establishing a Republic instead of a Democracy (as reviewed in the link video, discussing the rule of law versus the majority).
James Madison reviews the downfalls of a large democracy in the Federalist Paper, No. 10: The Utility of the Union as a Safeguard Against Domestic Faction and Insurrection.
The public today is often bombarded with reports, news (non-news) - an overabundance of opinions regarding important issues. Without the basic understanding of the U.S. Republic, individuals have been conditioned to react with and vote based on emotion, as opposed to thoughtful reasoning; the breaking down of issues with intelligent discourse based on Constitutional understanding.
Authors have broken down a differentiation of a democracy in the simplest term as a majority dictating issues. When a majority of persons are swayed with emotion, it is ‘mob rule’. This distinction is important, as more and more voters are craving socialism, with groups such as ANTIFA and #xyzMOVEMENTS continuing to form. The Founding Fathers researched all the various forms of governments thoroughly before specifically establishing a Republic instead of a Democracy (as reviewed in the link video, discussing the rule of law versus the majority).
James Madison reviews the downfalls of a large democracy in the Federalist Paper, No. 10: The Utility of the Union as a Safeguard Against Domestic Faction and Insurrection.
"The second expedient is as impracticable as the first would be unwise. As long as the reason of man continues fallible, and he is at liberty to exercise it, different opinions will be formed. As long as the connection subsists between his reason and his self-love, his opinions and his passions will have a reciprocal influence on each other; and the former will be objects to which the latter will attach themselves. The diversity in the faculties of men, from which the rights of property originate, is not less an insuperable obstacle to a uniformity of interests. The protection of these faculties is the first object of government. From the protection of different and unequal faculties of acquiring property, the possession of different degrees and kinds of property immediately results; and from the influence of these on the sentiments and views of the respective proprietors, ensues a division of the society into different interests and parties.
The latent causes of faction are thus sown in the nature of man."
The latent causes of faction are thus sown in the nature of man."
A great deal of emphasis has been placed on the importance of the 2018 mid-term elections, and the tide of ‘Red’ versus ‘Blue’ control at State and Federal levels. In Arizona, two candidates posted the following in the election overview of candidates:
Taking the importance to the Nth degree for properly educating and understanding the foundations and ideologies of a Republic versus a Democracy: A democracy may vote in socialism; the U.S. Republic cannot, because representatives must abide by the guaranteed protections within the Constitution, especially our Rights.
- Steve Gaynor (Republican) for AZ Secretary of State: “… bedrock of our democracy …”
- Katie Hobbs (Democrat) for State Senator: “… foundation of our democracy …”
Taking the importance to the Nth degree for properly educating and understanding the foundations and ideologies of a Republic versus a Democracy: A democracy may vote in socialism; the U.S. Republic cannot, because representatives must abide by the guaranteed protections within the Constitution, especially our Rights.
PART 2 of 4: What is a Right? Why Healthcare is Not a Right.
As previously written in Part I: The A, B, C of U.S. Governance, unless voters understand elementary basics of governance, they will be unable to have reasoned, intelligent decision making when reviewing issues and voting. Educating the public that the majority rules, a Democracy, fosters politicians swaying large groups of a divided population with emotion – known as mob rule - versus lawful thought and discourse in a Republic governed by the Constitution.
| Question 1: "What is the Constitution?" The most basic, succinct answer is that it’s the document protecting our Rights from the government, Rights it cannot take away. The Founding Fathers Alexander Hamilton, John Jay, and James Madison wrote about the rationale behind the establishment of the Constitution, with the general insights:
| Question 2: "What is a Right?" The first Rights established in the Declaration of Independence in 1776: “All men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness — That to secure these rights, Governments are instituted among Men … Therefore, when groups use the current statement healthcare is a Right (or a human Right); there is a general lack of understanding regarding the term. The Bill of Rights is the continuation of all Rights naturally afforded to citizens that the government cannot take away; not Rights to be supplied by the government. Rights are Inalienable from God, fundamental rights not transferable or impossible to take away. These rights include the life, liberty, and the pursuit of happiness, the right of privacy, to travel, and have possessions. |

Veterans are the citizens who have the Right to free healthcare through the Veterans Affairs (VA), for wounds or illnesses sustained in the protection of the country. The inefficiency of the VA system as a government run entity has sadly been well documented over the last two decades, and requires separate coverage of its own.
The concept of a Right given by the government is an oxymoron, being the very essence of Unconstitutional. Rights define our freedom from the government. When Rights are given to, allowed control by the government, it is socialism. And, Socialism is defined in Merriam-Webster as:
economic and political theories advocating collective or governmental ownership and administration of the means of production and distribution of goods (and services); there is no private property; a system which the means of production are owned and controlled by the state; a stage of society in Marxist theory transitional between capitalism and communism.
There is currently a growing trend calling for a single healthcare payer: That single payer is the government. Giving full, nonmilitary healthcare control over to the government is contrary to having Rights, often called socialized medicine, which is in actuality what I term healthcare socialism.
The concept of a Right given by the government is an oxymoron, being the very essence of Unconstitutional. Rights define our freedom from the government. When Rights are given to, allowed control by the government, it is socialism. And, Socialism is defined in Merriam-Webster as:
economic and political theories advocating collective or governmental ownership and administration of the means of production and distribution of goods (and services); there is no private property; a system which the means of production are owned and controlled by the state; a stage of society in Marxist theory transitional between capitalism and communism.
There is currently a growing trend calling for a single healthcare payer: That single payer is the government. Giving full, nonmilitary healthcare control over to the government is contrary to having Rights, often called socialized medicine, which is in actuality what I term healthcare socialism.
PART 3 of 4: Single Payer = Government, Healthcare Socialism
The American system has been based upon freedom, the free market, at its very core. Healthcare is included with the exception of the Veterans Affairs (VA) system, and the formation of Medicare, and now the expansion of Medicaid. A growing trend in the country is a call for a single payer healthcare system.
Recent articles have cited a high percent (up to 40%) of medical students wanting a single payer. This year, Medical students bring the AMA into the single payer dialogue AMA House of Delegates 2018 Annual Meeting, June 9-13, 2018
Well, who is that payer? The answer is the government. What would be the single payer system - VA, Medicare, Medicaid? I suggest we not use the term single payer system, and instead delineate the true description, what I refer to as healthcare socialism.
As discussed in Part I of this series, the Federal Government was designed for protection of the Constitution, and to be effective with limited power, operating with efficiency. Government run healthcare has proven to not have limited power, to be costly with decreased quality, and to be inefficient.
Recent articles have cited a high percent (up to 40%) of medical students wanting a single payer. This year, Medical students bring the AMA into the single payer dialogue AMA House of Delegates 2018 Annual Meeting, June 9-13, 2018
Well, who is that payer? The answer is the government. What would be the single payer system - VA, Medicare, Medicaid? I suggest we not use the term single payer system, and instead delineate the true description, what I refer to as healthcare socialism.
As discussed in Part I of this series, the Federal Government was designed for protection of the Constitution, and to be effective with limited power, operating with efficiency. Government run healthcare has proven to not have limited power, to be costly with decreased quality, and to be inefficient.
The following cases are only a few of the major healthcare fraud cases over the last few years:
Healthcare socialism includes physicians as employees of the hospitals, ergo employees of the government. Under the current government payer system, Hospital-employed physicians drain Medicare By Alex Kacik|November 14, 2017
1 National Health Care Fraud Takedown Results in Charges against 301 Individuals for Approximately $900 Million in False Billing, Department of Justice, June 22, 2016, https://www.justice.gov/opa/pr/national-health-care-fraud-takedown-results-charges-against-301-individuals-approximately-900
2 Justice Department charges three in $1 billion Medicare fraud scheme, The Wall Street Journal, July 22, 2016, http://www.foxnews.com/politics/2016/07/22/justice-department-charges-three-in-1-billion-medicare-fraud-scheme.html
3 U.S. Charges 412, Including Doctors, in $1.3 Billion Health Fraud, The New York Times, July 13, 2017, https://www.nytimes.com/2017/07/13/us/politics/health-care-fraud.html
4 Beverly Woman Defrauded State Of $1 Million From Medicaid: Prosecutors, DNAinfo, October 14, 2017, https://www.dnainfo.com/chicago/20171018/beverly/santila-terry-speech-therapy-clinic-theft-charges-docbarbie-hair-boutique/
- 301 National take down in healthcare fraud results in approximately $900 million in false billing1
- Three charged in $1B Medicare fraud scheme2
- 412, including doctors, in $1.3 Billion Health Fraud3
- Woman defrauds Medicaid of $1 Million4
Healthcare socialism includes physicians as employees of the hospitals, ergo employees of the government. Under the current government payer system, Hospital-employed physicians drain Medicare By Alex Kacik|November 14, 2017
1 National Health Care Fraud Takedown Results in Charges against 301 Individuals for Approximately $900 Million in False Billing, Department of Justice, June 22, 2016, https://www.justice.gov/opa/pr/national-health-care-fraud-takedown-results-charges-against-301-individuals-approximately-900
2 Justice Department charges three in $1 billion Medicare fraud scheme, The Wall Street Journal, July 22, 2016, http://www.foxnews.com/politics/2016/07/22/justice-department-charges-three-in-1-billion-medicare-fraud-scheme.html
3 U.S. Charges 412, Including Doctors, in $1.3 Billion Health Fraud, The New York Times, July 13, 2017, https://www.nytimes.com/2017/07/13/us/politics/health-care-fraud.html
4 Beverly Woman Defrauded State Of $1 Million From Medicaid: Prosecutors, DNAinfo, October 14, 2017, https://www.dnainfo.com/chicago/20171018/beverly/santila-terry-speech-therapy-clinic-theft-charges-docbarbie-hair-boutique/
- A 49% increase in hospital-employed physicians between 2012 and 2015 led to a $3.1 billion increase in Medicare costs related to four specific procedures in cardiology, orthopedics and gastroenterology, according to analysis from consulting firm Avalere Health.
- Medicare paid $2.7 billion more for diagnostic cardiac catheterizations, echocardiograms, arthrocentesis and colonoscopies delivered in hospital outpatient settings than it would for treatment in independent facilities, while beneficiaries footed a $411 million higher bill.
- Hospital-employed physicians performed more services in costlier hospital outpatient settings, resulting in up to 27% higher costs for Medicare and 21% for patients.
How would it be funded initially as there is no long term sustainability.
The existing Federal Total revenue as of 2018 is only $3.654 trillion (T)
| The current US Debt Clock as of August 2018 reads:
|  |
Right now, the country cannot fund social security or existing Medicare (and Medicaid which is not included or considered). The Forbes July 9, 2018 article reviewed the additional cost projections of a single payer system:
- An independent analysis of Sanders's plan conducted by the left-leaning Urban Institute estimated that it would cost $32 trillion over 10 years.
- And those are just the financial costs. Socialized medicine's human costs are even greater. Single-payer systems, the world over, ration care and force patients to wait for treatment.
- The United States can barely afford its existing healthcare obligations. In 2017, the federal government spent more than $700 billion on Medicare -- a 65 percent increase over just 10 years.
It is important to read all three sections of this series to appreciate under Healthcare Socialism, the individual gives up their Rights because the government dictates: what is to be done, the services to be given, lack of financial responsibility with a non-sustainable system, and who is to do what job where and when – which is covered in the next section.
PART 4 of 4: Under Healthcare Socialism
A major factor that is never discussed in healthcare socialism (since it is referred to as ‘single payer’) is the education of clinician staff - the doctors, nurses, etc. which is not covered regarding cost and decreased quality.
New York University (NYU) just announced they now have a tuition free medical school. In response, Elisabeth Rosenthal, MD, editor-in-chief of Kaiser Health News, explains why NYU got it wrong.
In an op-ed for The New York Times, Dr. Rosenthal, a former emergency room physician, cites research that shows medical school debt often discourages students from pursuing lower-paying specialties or from practicing in areas where the majority of patients are on Medicaid.
Instead, students are more likely to pursue more highly paid specialties, like neurosurgery or orthopedic surgery.
By eliminating tuition … She claims most physicians who enter higher-paying specialties are able to quickly pay off their student loans; the physicians that have trouble doing so are those who opt to take lower salaries as primary care physicians …"Instead of making medical school free for everyone, NYU — and all medical schools — should waive tuition only for those students who commit to work where they are needed most," she wrote. (See Title V of the ACA tax law passed under Obama.)
New York University (NYU) just announced they now have a tuition free medical school. In response, Elisabeth Rosenthal, MD, editor-in-chief of Kaiser Health News, explains why NYU got it wrong.
In an op-ed for The New York Times, Dr. Rosenthal, a former emergency room physician, cites research that shows medical school debt often discourages students from pursuing lower-paying specialties or from practicing in areas where the majority of patients are on Medicaid.
Instead, students are more likely to pursue more highly paid specialties, like neurosurgery or orthopedic surgery.
By eliminating tuition … She claims most physicians who enter higher-paying specialties are able to quickly pay off their student loans; the physicians that have trouble doing so are those who opt to take lower salaries as primary care physicians …"Instead of making medical school free for everyone, NYU — and all medical schools — should waive tuition only for those students who commit to work where they are needed most," she wrote. (See Title V of the ACA tax law passed under Obama.)
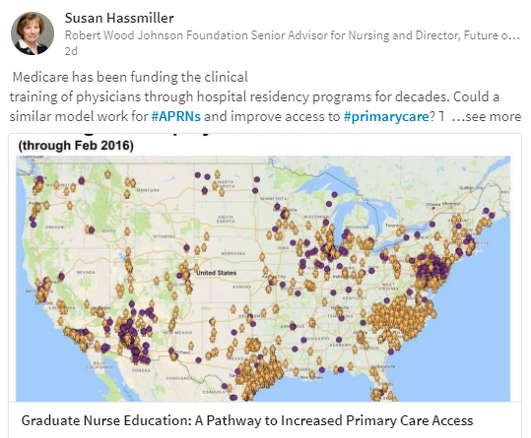
The ACA Tax Law (we need to stop calling it Obamacare, it is a tax law) has a lack of understanding, or misrepresentation, because it is not even read in entirety for the ability to even debate, and needs for repeal,
ACA, Page 1309, Title V SEC. 5207. FUNDING FOR NATIONAL HEALTH SERVICE
… authorized to be appropriated, out of any funds in the Treasury not otherwise appropriated, the following:
‘‘(1) For fiscal year 2010, $320,461,632.
‘‘(2) For fiscal year 2011, $414,095,394.
‘‘(3) For fiscal year 2012, $535,087,442.
‘‘(4) For fiscal year 2013, $691,431,432.
‘‘(5) For fiscal year 2014, $893,456,433.
‘‘(6) For fiscal year 2015, $1,154,510,336.
‘‘(7) For fiscal year 2016, and each subsequent fiscal year, the amount appropriated for the pre-ceding fiscal year adjusted by the product of ‘‘(A) one plus the average percentage increase in the costs of health professions education during the prior fiscal year; and ‘‘(B) one plus the average percentage change in the number of individuals residing in health professions shortage areas designated under section 333 during the prior fiscal year, relative to the number of individuals residing in such areas during the previous fiscal year.”
In summary, $BBs funneling out without oversight or budgeting and funding of bodies through schools without quality education, and then dictating who must work where and when.
The ACA is predominately discussed in regards to healthcare coverage for uninsured, some $17M people, because people choose to not make the time to actually read the whole Tax Law. As Title V reflects, monies being spent have nothing to do with coverage, and is shows spending with no accountability, and we are seeing negative outcomes with the reduced training and preparedness as clinicians – clinical time and sciences replaced with diversity, global health issues, nursing theory. Last year, I was interviewed by a university with a ‘leading nursing college’, asking me if people who would make good nurses are prevented from becoming nurses because they cannot pass basic sciences, so we just need to reduce more of the sciences as “they don’t use that knowledge anyways, right?”
… authorized to be appropriated, out of any funds in the Treasury not otherwise appropriated, the following:
‘‘(1) For fiscal year 2010, $320,461,632.
‘‘(2) For fiscal year 2011, $414,095,394.
‘‘(3) For fiscal year 2012, $535,087,442.
‘‘(4) For fiscal year 2013, $691,431,432.
‘‘(5) For fiscal year 2014, $893,456,433.
‘‘(6) For fiscal year 2015, $1,154,510,336.
‘‘(7) For fiscal year 2016, and each subsequent fiscal year, the amount appropriated for the pre-ceding fiscal year adjusted by the product of ‘‘(A) one plus the average percentage increase in the costs of health professions education during the prior fiscal year; and ‘‘(B) one plus the average percentage change in the number of individuals residing in health professions shortage areas designated under section 333 during the prior fiscal year, relative to the number of individuals residing in such areas during the previous fiscal year.”
In summary, $BBs funneling out without oversight or budgeting and funding of bodies through schools without quality education, and then dictating who must work where and when.
The ACA is predominately discussed in regards to healthcare coverage for uninsured, some $17M people, because people choose to not make the time to actually read the whole Tax Law. As Title V reflects, monies being spent have nothing to do with coverage, and is shows spending with no accountability, and we are seeing negative outcomes with the reduced training and preparedness as clinicians – clinical time and sciences replaced with diversity, global health issues, nursing theory. Last year, I was interviewed by a university with a ‘leading nursing college’, asking me if people who would make good nurses are prevented from becoming nurses because they cannot pass basic sciences, so we just need to reduce more of the sciences as “they don’t use that knowledge anyways, right?”
Accountable and responsible citizens are again required to maintain a well run and responsible Republic – beginning with every Representative reading in full all Bills, with the ability to discuss well thought out long and short term ramifications of ALL components. And, if Representatives feel that “We need to pass it in order to find out what is in it;” then it is up to Citizens to actually read, vote out all persons not representing their best interests – with the ACA Tax Law (we should not refer to as Obamacare) as the preeminent example of why. The U. S. Constitutional Republic does not have the means, nor want Healthcare Socialism. To understand in detail why not, perhaps we need to bring back Arthur J. Stansbury’s Catechism on the Constitution (Boston 1828) as required reading for all grade school children – and members of Congress.

| As the dark side of IVF slowly comes into focus, even more transparency is needed by Pamela Mahoney Tsigdinos, July 27, 2018 |  |
There are pitfalls with IVF that are not discussed. And, this business end of reproduction is more often than not cash only. There are virtually ZERO long term studies regarding what effect-impact freezing, and a host of other ‘things’, that are done to the egg, or sperm, or the embryos that have (or could have) on the child that is produced. This 'miracle of modern medicine' could be good ... or just OK ... or it could be very, very bad. Science has rubbed the lamp and we cannot put the genie back in the bottle. After counseling many women in my career, the great emotional toil let alone the finances are not discussed. The ethical check is also missing regarding instances of doctors using their own sperm such as the Indiana doctor who in 2016 used his own sperm at least 50 times.
As the character Dr. Ian Malcom (played by Jeff Goldblum) said in the 1993 movie Jurassic Park, “Your scientists were so preoccupied with whether they could (create life) that they didn’t stop to think if they should.” by Karen F., (Ret) RN, NP OB & Palliative Care

by Rose Rohloff
A Memorial Day quote yesterday regarding veterans also exemplifies much of what has happened in healthcare over the last 10 years, regarding the focus on Population Health, meaningful use reporting, value based analysis, big data analytics-claims data, and mergers of health systems with large EMRs, with focus on reporting.
“We are arguing over a statistical analysis. This is the challenge that we face in society today ,,, we are quantifying numbers because it’s easy to look at a number, and it’s not easy to look at the value of a human life. I would say to you today that (losing) one a day, one a year is too many.”
Kyle Reyes, CEO, The Silent Partner Marketing
Kyle Reyes, CEO, The Silent Partner Marketing
When the primary focus is on data (the multiple of numbers/records-statistics), singular records and numbers or outliers are not worth the time and effort of analysts and executives. And yet, they should be as each record is a real patient, a friend, a loved one.
The solution is bringing analysis down to the most base level of management with front line analysis, to coincide with first-hand observation, the voice of the patient & their caregivers/champions, and reducing the ever growing administrative overhead. Bigger is not better for addressing health and care of populations, when the focus is shifted upward with large systems where individuals are lost: Especially when the individual issues are indicative of the core problems that need to be addressed for quality care delivery.
The need for P&P Reviews
The solution is bringing analysis down to the most base level of management with front line analysis, to coincide with first-hand observation, the voice of the patient & their caregivers/champions, and reducing the ever growing administrative overhead. Bigger is not better for addressing health and care of populations, when the focus is shifted upward with large systems where individuals are lost: Especially when the individual issues are indicative of the core problems that need to be addressed for quality care delivery.
The need for P&P Reviews

by Rose Rohloff

Naloxone is an emergency medication; it is temporary and doesn't stop or eliminate opioid abuse, addiction.
This week, reports were released in the media that US homes need Narcan to aid in opioid overdose epidemic, surgeon general advises
This week, reports were released in the media that US homes need Narcan to aid in opioid overdose epidemic, surgeon general advises
Dr. Delos Marshall "Toby" Cosgrove, the previous CEO of Cleveland Clinic, spoke to a room of healthcare leaders from across the country about the Opioid Crisis in April 2017. The discussion centered around the abuse of taking prescribed medications - legally and illegally - with the current trend of NARC Parties. He explained that NARC Parties entail the supply of Naloxone (the common brand name is Narcan, used by hospital-emergency personnel as the medication to temporarily counteract a narcotic or heroine overdose.) He continued that having Naloxone allowed people to overdose, the person(s) were then given Narcan in order to continue partying.
The general public needs to be aware: Naloxone has been reported to foster increased abuse of drugs by allowing revival of overdosing for continuing to take more drugs. Naloxone is the generic of Narcan. Just as EpiPen is only the delivery system and not the generic drug Epinephrine, It is important to know the difference between the brand name versus the generic drug name.
The general public needs to be aware: Naloxone has been reported to foster increased abuse of drugs by allowing revival of overdosing for continuing to take more drugs. Naloxone is the generic of Narcan. Just as EpiPen is only the delivery system and not the generic drug Epinephrine, It is important to know the difference between the brand name versus the generic drug name.
The danger of advising the untrained public to distribute emergency medicine
"A serious problem is many doctors and many more nurses are unaware of the different mode of metabolism of Fentanyl and Methadone. With various dosages of Fentanyl and Heroin or combinations of other opioids, the efficacy of Naloxone or Naltrexone is compromised. The general public (let alone many new doctors and nurses) do not have a working understanding of the differences in these competitive antagonists." "There may not be any impact for at least 30 minutes with a basic spray." 45 year RN, BSN, NP, MSN, Committee Member Opioid Crisis, Board of Directors Health Facility
Many clinicians, let alone the general public, are not specifically trained in the proper dosage and treatment with Naloxone for the various forms and dosages of opioids and heroin.
FDA Advisory Committee on the Most Appropriate Dose or Doses of Naloxone to Reverse the Effects of Life-threatening Opioid Overdose ... Sept 2016
"The effectiveness of naloxone, and thus the exposure required, will depend on the opioid dose, the potency of the opioid in binding receptors, the lipophilicity of the opioid in crossing into the CNS system and the elimination half-life of the opioid, together with patient factors (7, 26). Appendix [2] and [2a] includes further information on naloxone pharmacology. The complex pharmacology of appropriate dosing is further compounded as often the fentanyl involved is illicitly manufactured without normal procedures or controls and may be introduced surreptitiously into heroin or prescription painkillers. Reports from the field confirm the need for additional naloxone doses to reverse opioid overdoses including those involving more potent fast onset synthetic opioids."
Many clinicians, let alone the general public, are not specifically trained in the proper dosage and treatment with Naloxone for the various forms and dosages of opioids and heroin.
FDA Advisory Committee on the Most Appropriate Dose or Doses of Naloxone to Reverse the Effects of Life-threatening Opioid Overdose ... Sept 2016
"The effectiveness of naloxone, and thus the exposure required, will depend on the opioid dose, the potency of the opioid in binding receptors, the lipophilicity of the opioid in crossing into the CNS system and the elimination half-life of the opioid, together with patient factors (7, 26). Appendix [2] and [2a] includes further information on naloxone pharmacology. The complex pharmacology of appropriate dosing is further compounded as often the fentanyl involved is illicitly manufactured without normal procedures or controls and may be introduced surreptitiously into heroin or prescription painkillers. Reports from the field confirm the need for additional naloxone doses to reverse opioid overdoses including those involving more potent fast onset synthetic opioids."
Narcan (Naloxone HCL) Use in Opiod Overdose: A Perspective
4/10/2018
by Joan M. Rider-Becker, BS, PharmD, FMPA
Retired, Emeritus Professor, Pharmacy Practice Ferris State University College of Pharmacy Education/Training
B.S. Pharmacy-Ferris State University College of Pharmacy-1987
Pharmacy Practice Residency-Bronson Hospital Kalamazoo, MI-1987-1988
Doctor of Pharmacy (PharmD), University of Michigan-College of Pharmacy Ann Arbor, MI 1990
An important point for the general public who is not used to or trained in emergency medicine, this “rescue” drug is only the first step in the opioid crisis ... not the end all and be all of treatment. I would like to respond to this “advisory report” from the Surgeon General as a pharmacist, an Emeritus Professor, Pharmacy Practice from a College of Pharmacy, former President/Chair of the Michigan Pharmacist Association (MPA) and Fellow of this Association; and lastly as a chronic pain patient.
I have used opioids now for chronic pain management after a car accident almost twenty-years ago. I will admit, I was taken aback by my family physician about a month ago being given a prescription for Narcan (generic name Naloxone) as a “precautionary measure” for my chronic opioid use. The form I was prescribed is a nasal formulation vs. the oral/injection form. When I took it to a pharmacy to be filled, I had to undergo “special counseling” by a pharmacist (even with my credentials) which consisted of a video on proper use and a warning that after use, 911 had to be called and I was to be taken to the emergency room for follow-up. This is the proper follow-up when someone is prescribed any rescue medication for a drug reaction. The Naloxone is only to be given when a known opioid (i.e. codeine and it’s derivatives; Fentanyl, Meperidine, etc...) is given or taken in life-threatening incidences. I was instructed, "Were you aware that Naloxone has two elimination half-lives because this drug has an active metabolite; and, were you aware that Naloxone and Naltrexone are different agents, but are easily confused."
I believe giving someone this agent for overdose situations is giving a false sense of security that nothing else needs to be done. Nasal Naloxone is like putting a bandage on a cut artery. You may stop the blood flow at the moment, but the wound will continue to bleed if the wound isn’t sutured properly. Without appropriate emergency room follow up of an opioid overdose the person may die from that overdose.
Many opioids vary in dose, strength, predictability and most of all drug half-life. Knowing the half-life of drugs is essential to know how long the drug is going to last in your body. Drug half-life’s, drug absorption, distribution and elimination is well covered in Colleges of Pharmacy in courses such as pharmacology, pharmacokinetics and pharmacotherapeutics. Pharmacists do not know the pharmacokinetics on every drug substance out there by memory, and we are called the drug experts. Physicians do not have nearly as much education on medications as pharmacists, yet they are the first line of treating drug overdoses in emergency situations along with the nurses, Physician Assistants and Nurse Practitioners.
The general public is being provided a false sense of security by the media to carry this drug in their homes to address the opioid crisis. The public needs to be AWARE there is more to treating an opioid overdose than just squirting this agent up their nose.
I have used opioids now for chronic pain management after a car accident almost twenty-years ago. I will admit, I was taken aback by my family physician about a month ago being given a prescription for Narcan (generic name Naloxone) as a “precautionary measure” for my chronic opioid use. The form I was prescribed is a nasal formulation vs. the oral/injection form. When I took it to a pharmacy to be filled, I had to undergo “special counseling” by a pharmacist (even with my credentials) which consisted of a video on proper use and a warning that after use, 911 had to be called and I was to be taken to the emergency room for follow-up. This is the proper follow-up when someone is prescribed any rescue medication for a drug reaction. The Naloxone is only to be given when a known opioid (i.e. codeine and it’s derivatives; Fentanyl, Meperidine, etc...) is given or taken in life-threatening incidences. I was instructed, "Were you aware that Naloxone has two elimination half-lives because this drug has an active metabolite; and, were you aware that Naloxone and Naltrexone are different agents, but are easily confused."
I believe giving someone this agent for overdose situations is giving a false sense of security that nothing else needs to be done. Nasal Naloxone is like putting a bandage on a cut artery. You may stop the blood flow at the moment, but the wound will continue to bleed if the wound isn’t sutured properly. Without appropriate emergency room follow up of an opioid overdose the person may die from that overdose.
Many opioids vary in dose, strength, predictability and most of all drug half-life. Knowing the half-life of drugs is essential to know how long the drug is going to last in your body. Drug half-life’s, drug absorption, distribution and elimination is well covered in Colleges of Pharmacy in courses such as pharmacology, pharmacokinetics and pharmacotherapeutics. Pharmacists do not know the pharmacokinetics on every drug substance out there by memory, and we are called the drug experts. Physicians do not have nearly as much education on medications as pharmacists, yet they are the first line of treating drug overdoses in emergency situations along with the nurses, Physician Assistants and Nurse Practitioners.
The general public is being provided a false sense of security by the media to carry this drug in their homes to address the opioid crisis. The public needs to be AWARE there is more to treating an opioid overdose than just squirting this agent up their nose.

| by Rose Rohloff  | Another common practice over the past decade is the prescription of broad spectrum antibiotics for non-life threatening conditions. Broad spectrum antibiotics are for use in life threatening conditions/sepsis when there is no time to wait for a culture, or the inability to do a culture. Broad spectrum antibiotics target the necessary bacteria needed in the adult intestinal tracts; and so, the standard practice has become the second prescribing for probiotics; the requiring of multiple medications to be taken. Additionally, numerous reports over the last 10 years have shown the continued misuse of antibiotics (e.g. CDC Grand Rounds) causing antibiotic resistance, with the need for more and more antibiotics to be created and used. |
What has caused the layering of medications
The country is currently facing increased antibiotic resistance, opioid crisis, etc. due to our culture being conditioned in the taking of medications versus alternative treatments, or prescriptions of medications without diagnosis. A mother of a small child was recently told by a doctor as part of her son's care, "It is very important for you to teach your child how to swallow pills. Start with candy sprinkles, then swallow mini M&Ms, and then have him swallow large M&Ms so he can take multiple pills at the same time." This instruction was given to the mother without a diagnosis for her son, no plan to achieve understanding of what was causing his pain to then create a plan of care - which may or may not have needed to include medication.
Consumer engagement is needed with all medications being prescribed to be fully empowered, to understand: 1) the need for prescriptions, why and when appropriate, 2) the side effects of medications to determine alternatives versus adding on more medications, and 3) to eliminate the misuse of medications without the continued layering of additional drugs. Antibiotics should only be used when the body, given time, cannot fight a severe bacterial infection. And, antibiotics should only be given out after a culture is performed to eliminate a virus as the cause, or to target the specific bacteria. Broad spectrum antibiotics should only be used with life threatening-septic issues while waiting for a culture, or there is not the ability to perform a culture.
Consumer engagement is needed with all medications being prescribed to be fully empowered, to understand: 1) the need for prescriptions, why and when appropriate, 2) the side effects of medications to determine alternatives versus adding on more medications, and 3) to eliminate the misuse of medications without the continued layering of additional drugs. Antibiotics should only be used when the body, given time, cannot fight a severe bacterial infection. And, antibiotics should only be given out after a culture is performed to eliminate a virus as the cause, or to target the specific bacteria. Broad spectrum antibiotics should only be used with life threatening-septic issues while waiting for a culture, or there is not the ability to perform a culture.
